ACG Clinical Guideline: Primary Sclerosing Cholangitis : Official journal of the American College of Gastroenterology
Preamble
The writing group was invited by the Practice Parameters Committee and the Board of the Trustees of the American College of Gastroenterology to develop a practice guideline on primary sclerosing cholangitis (PSC).
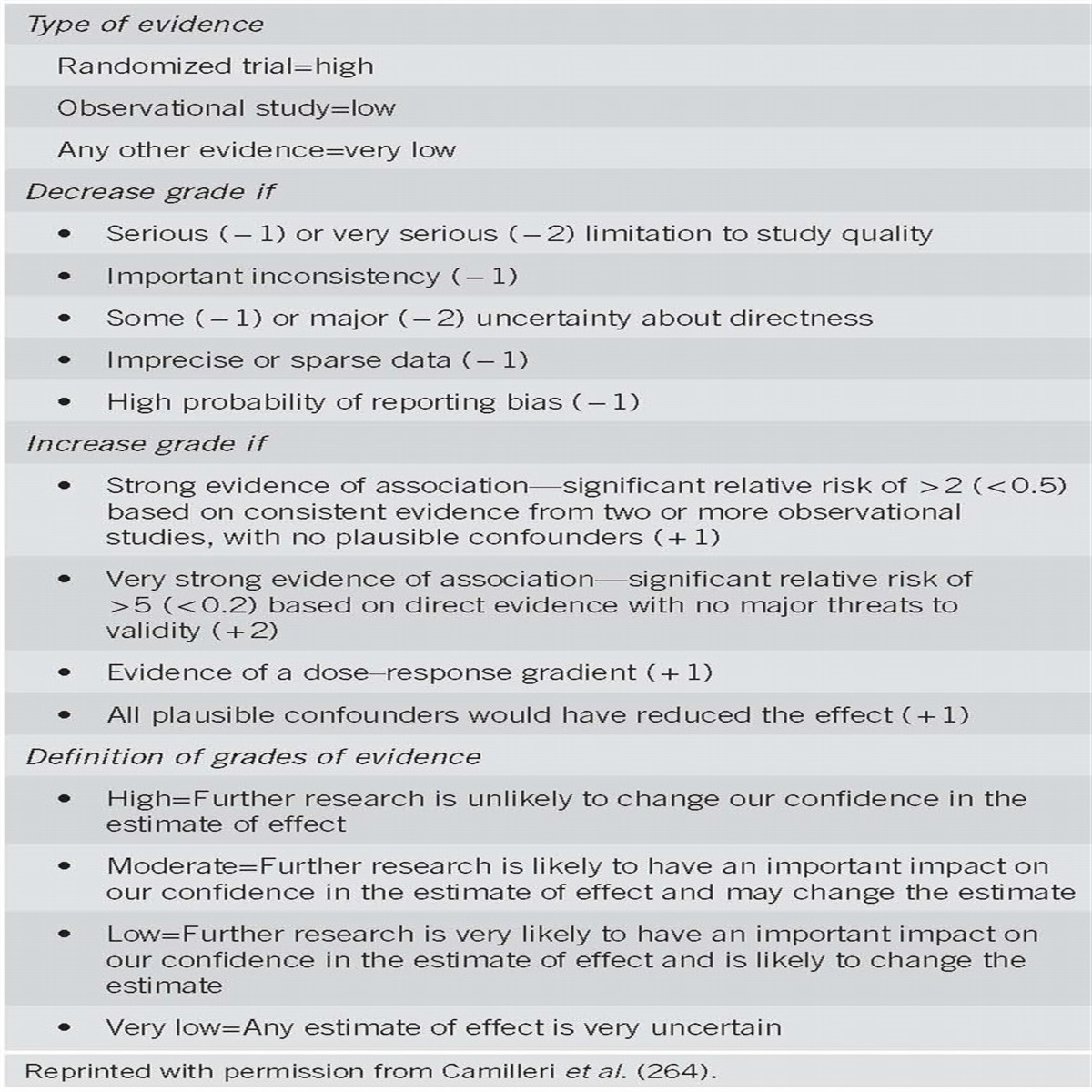
Guidelines for clinical practice are intended to indicate preferred approaches to medical problems as established by scientifically valid research. Double-blind, placebo-controlled studies are preferable, but reports and expert review articles are also used in a thorough review of the literature conducted through the National Library of Medicine’s MEDLINE. When only data that will not withstand objective scrutiny are available, a recommendation is identified as a consensus of experts. Guidelines are applicable to all physicians who address the subject, without regard to specialty training or interests, and are intended to indicate the preferable but not necessarily the only acceptable approach to a specific problem. Guidelines are intended to be flexible and must be distinguished from standards of care that are inflexible and rarely violated. Given the wide range of specifics in any healthcare problem, the physician must always choose the course best suited to the individual patient and the variables in existence at the moment of decision.
Guidelines are developed under the auspices of the American College of Gastroenterology and its Practice Parameters Committee, and are approved by the Board of Trustees. Each has been intensely reviewed and revised by the Committee, other experts in the field, physicians who will use them, and specialists in the science of decision of analysis. The recommendations of each guideline are therefore considered valid at the time of their production based on the data available. New developments in medical research and practice pertinent to each guideline will be reviewed at an established time and indicated at publication, to assure continued validity.
INTRODUCTION
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver and biliary tract disease that has a highly variable natural history (1). The pathogenesis of the disorder remains elusive, although the complications of the disease are a direct result of fibrosis and strictures involving intra and extrahepatic bile ducts (1). PSC may be asymptomatic for long periods but may also have an aggressive course, leading to recurrent biliary tract obstruction, recurrent episodes of cholangitis, and may progress to end-stage liver disease. The diagnosis is now most frequently established using magnetic resonance cholangiography (MRCP), although direct cholangiography may be more sensitive (2). The typical cholangiographic findings include focal stricturing and saccular dilatation of the bile ducts, which may lead to a “beaded” appearance (3).
The differential diagnosis of PSC includes several disorders that lead to biliary strictures such as bacterial cholangitis, intraarterial administration of floxuridine, prior biliary surgery, and AIDS-related cholangiopathy (3).
Definition
PSC is an idiopathic condition defined as the presence of beading and stricture formation of the intra and/or extrahepatic bile ducts that cannot be ascribed to another cause, thus differentiating PSC from secondary sclerosing cholangitis (1, 3, 4, 5). Many, if not most, cases of PSC are associated with inflammatory bowel disease (IBD) (1, 6, 7, 8). Therefore, PSC is a diagnosis of exclusion that can be established only in the absence of toxic, infectious, or inflammatory processes, which may lead to the characteristic bile duct injury pattern (1).
Epidemiology
The prevalence and incidence of PSC varies in different series from different regions of the world. The prevalence of PSC in ulcerative colitis has been estimated to be ˜5%. A survey in Sweden of 1,500 patients with ulcerative colitis found that 5% had an elevated alkaline phosphatase (ALP); the diagnosis of PSC was confirmed in 55 patients, a prevalence of 3.7% (9). PSC was also more common in men and those with pancolitis compared with those with left-sided colitis or proctitis (5.5% vs. 0.5%). A recent study found that approximately two-thirds of a cohort of 579 patients had IBD, three-quarters had ulcerative colitis, and the majority had pancolitis (6). The prevalence of IBD among Asian and Southern European populations with PSC is estimated to be 30%–50% (1). Based on these data, the prevalence of PSC in the United States has been estimated to be in the range of 1 to over 16 per 100,000 (1). It is possible that the true prevalence of PSC may be higher or lower than these estimates, because cholangiography may not be frequently performed, may fail to identify all cases, and as many patients with PSC may have normal serum ALP.
Gender: Approximately 60%–70% of patients with PSC and UC are men, and age at diagnosis is usually 30–40 years (1). Among patients without UC, there is a slight female predominance.
Pathogenesis
The cause of PSC remains elusive, although there have been several large-scale genome-wide association studies that have identified genotypic associations in cohorts with PSC (1, 10, 11, 12). Similarly, characteristic human leukocyte antigen haplotype associations have long been recognized in PSC (1, 13, 14). In addition, the strong association between PSC and IBD points to a possible role of autoimmunity (1). Other putative causes for PSC have been suggested, such as mutations in the gene encoding the cystic fibrosis transmembrane receptor and recurrent bacterial infections (1, 15, 16, 17, 18). The most plausible explanation for the pathogenesis of PSC is immunologic priming in a genetically pre-disposed individual, leading to the characteristic phenotype, possibly confounded by other host or exogenous factors (19).
DIAGNOSIS

The diagnosis of PSC is generally made in the setting of chronic cholestatic liver test abnormalities, in particular elevations of serum ALP level, along with cholangiograpic evidence of multifocal strictures of the intrahepatic and extrahepatic bile ducts, which may involve the intrahepatic or extrahepatic duct, or both (3). A liver biopsy, if performed, will show changes consistent will PSC (29). The characteristic “onion skin” fibrosis, which is almost pathognomonic for the disease, is seen infrequently (30). Furthermore, liver biopsy is seldom required to establish the diagnosis (21).
Signs and Symptoms
A large number of patients present without symptoms and come to attention simply by a finding of persistently abnormal liver tests. When symptoms occur, fatigue maybe the most commonly noted finding but it is nonspecific. Sudden onset of pruritus should signal the possibility of obstruction of the biliary tree. Other symptoms are those of advanced liver disease such as jaundice or gastrointestinal bleeding. Many patients with PSC may have IBD; hence, bleeding from the colon should lead to consideration of IBD as well as bleeding from portal hypertension. Abdominal distention with fluid and confusion are late symptoms, as is jaundice. Some patients may have fever and pain arising from cholangitis and other patients experience chronic right upper quadrant discomfort; however, right upper quadrant pain is not a prominent feature of PSC.
Biochemical Tests
Blood tests usually show a cholestatic profile with predominate elevation of ALP level. Gamma-glutamyl transferase will be elevated if obtained and the aminotransferases are often times only modestly elevated. Bilirubin and albumin levels are often normal at the time of diagnosis, although these levels may become increasingly abnormal as the disease progresses. Hypergammaglobulinemia is not a common finding, although IgM levels are found to be increased in ˜50% of patients (31). In recent years, elevations of serum levels of IgG4 have been found in ˜10% of patients with PSC and may represent a distinct subset (26, 27, 28). The patients who have elevated IgG4 levels tend to have a more rapidly progressive disease in the absence of treatment. Unlike patients with typical PSC, patients with IgG4-associated disease and PSC do appear to respond to corticosteroids (26, 32). All patients with PSC should be tested at least once for elevated serum IgG4 levels (26, 27, 28).
Autoantibodies
Autoantibodies can also occur in patients with PSC but the antimitochondrial antibody characteristic of primary biliary cirrhosis is not found. Anti-smooth muscle and antinuclear antibodies, as well as antineutrophil cytoplasmic antibodies can be found (33, 34, 35, 36). In some series, these have been present in >50% of patients; however, antineutrophil cytoplasmic antibodies and antinuclear and anti-smooth muscle antibodies are not specific for PSC.
Imaging
Imaging of the biliary tract is the most important initial step. Cross-sectional imaging, usually with ultrasound, computed tomography or magnetic resonance imaging will be performed in the patient with persistent cholestatic liver tests to exclude biliary obstruction. If obstruction is not found, then cholangiography is usually the next step. ERCP had been the diagnostic procedure of choice; however, in the past decade MRCP has rapidly supplanted ERCP as the preferred method of cholangiography for suspected PSC (4, 5, 20). MRCP is noninvasive, less expensive than ERCP, and has no associated risk of pancreatitis (20). MRCP, however, does not allow sampling of strictures for brush cytology or biopsy, nor does it allow therapeutic interventions if a mechanical reason for obstruction is found such as stone, stricture, or tumor.
Liver Biopsy
Liver biopsy is now seldom done to establish the diagnosis of PSC (21) and is generally not considered necessary to establish the diagnosis. There are, however, some patients who have normal cholangiograms but have suspected small duct PSC due to otherwise unexplained cholestastic liver tests; liver biopsy is necessary to confirm this diagnosis (22, 23, 24). The characteristic feature of liver biopsy, a periductal concentric “onion skin” fibrosis, is seldom found. Most often, the liver biopsy is interpreted as “compatible” with PSC.
Small Duct PSC
Small duct PSC makes up ˜5% of the entire spectrum of patients with PSC. The macroscopic bile ducts in small duct PSC are normal; hence, cholangiography will not be revealing. Diagnosis of small duct PSC requires liver biopsy, to demonstrate the characteristic microscopic disease. Interestingly, a number of patients with small duct PSC may later develop classic bile duct changes of large duct disease. The risk of progression from small duct PSC to classic disease is unknown (22, 23, 24).
Differential Diagnosis Of PSC
The differential diagnosis of PSC includes secondary sclerosing cholangitis, which may arise from prior biliary surgery, and cholangiolithiasis (Figure 1). Biliary strictures arising in HIV infection, IgG4, and cholangiocarcinoma, all fall into the differential diagnosis and can be difficult to distinguish from PSC itself (37, 38, 39, 40, 41). Other conditions with differential diagnosis are listed in Table 1.

Differential diagnosis of primary sclerosing cholangitis

Management of primary sclerosing cholangitis.
MEDICAL TREATMENT
At this time, there is no established medical treatment for patients with PSC.

UDCA
UDCA has been the best studied of a number of potential treatments. A study of 105 patients using the dose of UDCA appropriate for patients with primary biliary cirrhosis (13–15 mg/kg/day) did show biochemical improvement but lack of evidence of clinical improvement (25). Subsequently, somewhat higher doses were tested and potential benefit was identified (43, 44). A large trial, which was nevertheless under enrolled, was reported from Scandinavia using a dose of 17–23 mg/kg/day. Biochemical improvement and important trends in clinical improvement were seen (45). The study enrolled only 63% of patients planned by power calculations; thus, the results were inconclusive. Recently, a large trial using a high dose of UDCA of 28–30 mg/kg/day was tested (46). Unfortunately, in this study the patients receiving the drug fared worse when compared with placebo, with substantially more adverse clinically important outcomes such as the need for transplantation and the development of varices. More recently, high doses of UDCA have been associated with an increased risk of colonic neoplasia in the settings of PSC and ulcerative colitis. At this point, no indication exists for using the higher doses of 28–30 mg/kg/day of UDCA (42).
More recently, several studies have shown that patients with PSC, who normalize liver biochemistries, whether this occurs spontaneously or more often with UDCA therapy, have a better prognosis. This has led some to revisit the issue of UCDA treatment for PSC; many practitioners are using a dose of ˜20 mg/kg/day, although data from well-controlled clinical trials are lacking (47, 48, 49).
Immunosuppressive and other Agents
Other treatments that have been tested without any obvious proven clinical benefit or improvement of liver biochemistries include:
- Azathioprine (50)
- Budesonide (51)
- Docosahexaenoic acid (52)
- Methotrexate (53, 54)
- Metronidazole (55)
- Minocycline (56)
- Mycophenolate mofetil (57)
- Nicotine (58)
- Pentoxifylline (59)
- Pirfenodone (60)
- Prednisolone (61)
- Tacrolimus (62)
- Vancomycin (63)
Vancomycin
There are case series data and anecdotal reports that oral vancomycin has been associated with marked improvement in clinical symptoms and liver biochemistries in some patients, in particular in the pediatric age group (63). No randomized clinical trials of antibacterial therapy have been performed to date. This is a promising area for future study.
ENDOSCOPIC MANAGEMENT

Biliary obstruction in PSC may develop at all levels of the biliary tree, from microscopic biliary ductules to the extrahepatic bile ducts, but endoscopic therapy is feasible only for the larger bile ducts. ERCP is reserved for patients with significant bile duct strictures localized to the extrahepatic and large intrahepatic bile ducts, which are described as dominant strictures. For selected patients with dominant strictures, endoscopic intervention relieves the complications of pruritus and cholangitis, allows early diagnosis of cholangiocarcinoma, and may lead to improved survival.
Definition
At cholangiography, dominant strictures are defined as stenoses measuring <1.5 mm in the common bile duct or <1.0 mm in the hepatic ducts (73). Dominant strictures are common at the initial clinical presentation of PSC and frequently will develop over the course of the disease. In a retrospective study of 125 patients, a dominant stricture was detected in 56/125 (45%) of patients at time of diagnosis (74). By following patients over a median of 7.1 years, another retrospective study demonstrated the development of new dominant strictures in 77/151 (51%) patients (75). Advancements in therapeutic endoscopy for PSC have focused on dominant strictures, because they are common and potentially amenable to endoscopic therapy by ERCP.
Benefits of Endoscopic Therapy
Endoscopic treatment of dominant strictures offers clinical benefit with diminished symptoms of pruritus or cholangitis, reduced cholestasis, and measureable improvement of strictures radiologically. The studies that reported these outcomes have been relatively small, uncontrolled, and retrospective, but their results have been generally favorable and reflect the experience of multiple academic centers managing almost 500 patients over several decades (64, 65). In a representative study from 1991, 35 patients with dominant strictures were treated by dilation with or without stent placement, and showed improvement in jaundice, reduced rates of hospitalization, and radiologic improvement of the strictures (66). Another retrospective study of 53 patients, published in 1995, also reported benefit from treatment of dominant strictures: 77% of patients had improvement in liver-related tests, symptoms, or cholangiograms after dilation, with or without stenting and stone extraction (67). In 2001, a report of 71 patients with dominant strictures treated endoscopically showed favorable results. This retrospective comparison of dilation alone vs. dilation with stenting showed a statistically significant lessening of jaundice in both treatment groups, and reduced fevers for those with dilation (68).
Endoscopic treatment of dominant strictures in PSC may be considered specifically for cholangitis. Cholangitis can be the initial presentation of PSC and occurs frequently during the course of disease (76). Recurrent cholangitis can contribute to progression of the disease. Dominant strictures are associated with biliary bacterial colonization and antibiotic therapy alone may not be sufficient to eradicate the bacteria (77). The persistence of this bacteriobilia may be clinically significant: greater numbers of bacterial isolates have been associated with a shorter interval to liver transplant (71). ERCP is employed routinely to treat cholangitis due to biliary obstruction in other clinical settings, such as biliary obstruction from stone disease or malignancy, and biliary decompression allows improved response to antibiotic treatment and prevention of recurrent cholangitis. Endoscopic treatment of dominant strictures in PSC similarly may allow more effective treatment of cholangitis. The increased risk of cholangitis as a complication of ERCP, however, does reduce the potential benefit of endoscopic therapy for this indication (78).
Endoscopic treatment of dominant strictures in PSC may improve prognosis. Chronic biliary obstruction leads to progressive hepatic fibrosis and cirrhosis, even in the absence of pre-existing liver disease. Dominant strictures in PSC contribute to bile outflow obstruction, and have been associated with reduced survival free of liver transplantation (79). Relief of biliary obstruction by endoscopic therapy can arrest and potentially reverse cholestatic injury to the liver (80). Endoscopic therapy for relief of biliary obstruction due to dominant strictures in PSC has not been evaluated by prospective studies, but two retrospective studies did show improved survival after endoscopic therapy as compared with survival predicted by the Mayo Risk Score. In the first study, 63 patients were treated by balloon dilation of dominant strictures and their 5-year observed survival was significantly greater than predicted survival (83% vs. 65%, respectively) (81). In the second study, 55 patients were treated with balloon dilation of dominant strictures, 5 patients were treated with stenting, and the outcomes were positive: the 5-year observed survival was significantly greater than predicted survival in the treated group (94% vs. 78%, respectively) (73). Endoscopic therapy for dominant strictures, however, is not uniformly supported. In a retrospective study of 125 patients with PSC, ERCP was performed without therapy, and there was no significant difference in cholestasis 1 year after cholangiography in the 56 patients with dominant strictures as compared with the 69 patients without dominant strictures (74). However, this study did not evaluate the potential benefit of endoscopic intervention for their patients with dominant strictures, but simply found that 1-year prognosis is not worse when dominant strictures were present (82).
Cholangiocarcinoma and Dominant Strictures
Cholangiocarcinoma must be considered in every patient with PSC and a dominant stricture, although the majority of these strictures will prove to be benign (83). In a series of 128 patients with PSC, 80/128 (63%) of patients had dominant strictures and 21/80 (26%) of patients with dominant strictures developed cholangiocarcinoma (84). Evaluation of dominant strictures discovered soon after the diagnosis of PSC is particularly important: among patients with cholangiocarcinoma, almost half of the malignancies were diagnosed within the first 4 months after initial diagnosis of PSC (85).
Endoscopic techniques to detect malignancy in dominant strictures routinely include brushings for cytology and biopsies for pathology. The specificity of these methods in detecting cholangiocarcinoma is very high, but their sensitivity has been reported below 30%, which limits their negative predictive value (69). The poor sensitivity of conventional diagnostic tools has led to considerable effort to enhance the diagnostic yield by employing newer technologies. FISH increases sensitivity to 64% from one cytology specimen and the presence of polysomy on two sequential specimens increases the positive predictive value to 69% (69, 70). Cholangioscopy allows direct biliary visualization and directed biopsies of the dominant stricture, which has been reported to increase sensitivity and specificity to >90% (86). Confocal laser microscopy has a very high reported sensitivity (98%) and moderate specificity (67%) for indeterminate strictures in general, but has not been studied specifically in dominant strictures in PSC (87) Intraductal ultrasound also may offer improved diagnostic yield, although it has not been widely adopted since its initial report for diagnosis of indeterminate strictures (88).
Endoscopic Techniques
Techniques employed for endoscopic treatment of dominant strictures in PSC are not well standardized. Case series support the benefit of dilation, stent placement, and combinations of these methods for treatment of dominant strictures. A review of multiple case series showed that stent placement can lead to more frequent complications of cholangitis than dilation alone, but stenting for short duration will reduce the risk of stent occlusion and may allow stenting without increased risk of cholangitis (68, 72). Bile duct stones frequently develop in PSC due to impaired bile outflow and bacterial overgrowth from biliary strictures. When intraductal stones are recognized, endoscopic dilation of obstructing strictures and stone extraction will reduce bile outflow obstruction. Cholangioscopy is used primarily to interrogate indeterminate strictures in an effort to enhance detection of cholangiocarcinoma, but has the additional benefit of detection of unrecognized bile duct stones (89).
Patients undergoing endoscopic therapy for PSC are at significantly increased risk of post-ERCP cholangitis (78). Cholangitis in PSC can be life-threatening due to inability to decompress intrahepatic areas of biliary obstruction and infection. Prophylactic antibiotic therapy is a rational precaution against post ERCP cholangitis. Preoperative antibiotics followed by a 3- to 5-day course post ERCP have been advised, using quinolones or cephalosporins, although no prospective studies have been performed to determine the best antibiotic choices (71).
Percutaneous Treatment
Percutaneous cholangiography for treatment of dominant strictures can be performed in PSC patients with altered anatomy that prevents successful ERCP, such as Roux-en-Y choledochojejunostomy or gastric bypass, or as a rescue therapy after failed endoscopic access. Percutaneous cholangiography is generally the second line of treatment after ERCP because of the risk of complications, including hepatic arterial injury, hemobilia, and cholangitis (90, 91, 92). Percutaneous cholangiography also requires placement of a percutaneous drain, which can be uncomfortable or difficult for the patient to manage. Percutaneous cholangiography is the primary choice of treatment for intrahepatic strictures that cannot be accessed by the retrograde approach or for very tight strictures that cannot be traversed by endoscopically placed wires or dilators. When percutaneous treatment is undertaken, the dominant stricture must be dilated adequately to prevent retrograde biliary flow and percutaneous bile leakage.
Surgical Management
Biliary reconstruction by biliary-enteric drainage allows prolonged clinical improvement, with resolution of jaundice and cholangitis, but has significant risk of cholangitis and increased rates of mortality (93). Post-operative scarring also increases the difficulty of liver transplantation. Surgical drainage procedures have largely been discontinued in favor of transplantation due to the superior outcomes of liver transplantation (94).
LIVER TRANSPLANTATION

Liver transplantation is the definitive treatment for patients with decompensated cirrhosis. The natural history of PSC is extremely variable but, in the absence of effective medical therapy for PSC, the median time for progression of disease from diagnosis until death or liver transplantation is 10–12 years (34, 97). Liver transplantation for PSC with a deceased donor organ offers 5-year survival of 80–85% (95, 98).
Priority to receive a donor liver from the United Network for Organ Sharing is established by the MELD score. The MELD score is calculated from the patient’s bilirubin, international normalized ratio and creatinine, which together create an objective measure of liver dysfunction that can be compared across different etiologies of liver disease. Liver transplantation offers survival benefit for patients with MELD score >15; however, MELD scores in most United Network for Organ Sharing regions must be considerably higher to achieve liver transplant due to scarcity of donor organs (99). For patients listed for transplant, who seek an alternative to waiting for a progressive increase in MELD score until a deceased donor becomes available, transplantation from a living donor is a viable option: patients undergoing living donor transplant for PSC have long-term outcomes that are comparable or superior to those undergoing deceased donor transplant (100).
In specific clinical circumstances, patients with PSC may be offered additional MELD points, to improve their priority for receiving a donor organ for liver transplantation. MELD exception points can be approved by the United Network for Organ Sharing Regional Review Board for the following indications:
- Recurrent episodes of cholangitis, with >2 episodes of bacteremia or >1 episode of sepsis (101).
- Cholangiocarcinoma <3 cm in diameter, without evidence of metastasis, undergoing treatment through an institutional review board-approved clinical trial.
- Intractable pruritus.
Recurrence of PSC after liver transplantation is relatively common, affecting as many as 20% of patients at 5 years after transplant (102). The majority of patients tolerate recurrent disease without significant morbidity or mortality, but progressive disease can occur in as many as one-third of patients with recurrent PSC (103).
PSC AND IBD

The prevalence of IBD in PSC is much higher than previously thought and recent reviews have stated that up to 80% of patients with PSC have IBD (3). It is possible that the prevalence may have been underestimated given that the colonic mucosa may frequently appear normal on endoscopic examination, although biopsies may disclose evidence of histologic colitis. A preliminary study in which rectosigmoid biopsies were routinely performed and histology reviewed by an expert pathologist suggested that the prevalence may be as high as 90% (96).
Timing of Diagnosis
The majority of patients with IBD and PSC have a known diagnosis of IBD before the diagnosis of PSC. However, PSC may be diagnosed after proctocolectomy for UC and IBD may be diagnosed after a liver transplant has been done for end-stage liver disease due to PSC (3). IBD in patients with PSC may frequently be asymptomatic and have a quiescent course. Therefore, a full colonoscopy with biopsies is recommended in patients with PSC regardless of the presence of symptoms. This recommendation is consistent with other PSC Practice Guidelines (3).
IBD in PSC: a Unique Phenotype
IBD among patients with PSC appears to be clinically distinct (1, 105). The disease presents earlier in life than in patients without PSC, is often quiescent, and may be asymptomatic; rectal bleeding is infrequent and there is a predilection for right-sided colitis with relative sparing of the rectum. Patients may experience long asymptomatic periods (105). “Backwash ileitis” is relatively common and patients may be more likely to develop pouchitis after ileo-anal anastomosis. Finally, the presence of portal hypertension in patients with IBD and PSC is associated with an increased risk of stomal and peristomal varices (1, 3). IBD associated with PSC may be ulcerative colitis or Crohn’s disease involving the colon, while isolated small-bowel Crohn’s disease is usually not associated with PSC (3). Many patients may have “indeterminate colitis” and may not be easily classified as having ulcerative colitis or Crohn’s disease of the colon (3, 105).
Based on these data, it is reasonable to recommend a full colonoscopy with random biopsies in patients with PSC, who do not already have a diagnosis of IBD. Biopsies should be obtained even if the colonic mucosa appears grossly normal. Some have advocated that colonoscopy with biopsy be repeated every 5 years, although there is no consensus on this approach.
Risk of Colonic Malignancy
The risk of colorectal dysplasia and cancer is significantly higher (approximately four- to fivefold) among patients with PSC and IBD compared with those with IBD without PSC (104). The mechanism for increased risk of colon cancer in PSC–IBD is unknown, but exposure of the colonic mucosa to toxic bile acids, namely secondary bile acids that may promote carcinogenesis such as deoxycholic acid, has been proposed (105). The possible favorable effect of low-dose UDCA in a few retrospective studies also has been thought to provide circumstantial evidence in support of the toxic bile acid hypothesis, although there are no prospective controlled trials demonstrating a benefit for UDCA for chemoprevention against colon dysplasia or neoplasia in IBD associated with PSC. A recent meta-analysis suggested a possible benefit for low-dose (8–13 mg/kg/day) UDCA but significant heterogeneity in the studies was notified, limiting the interpretation of the results (106). 5-Acetylsalicylic acid may also reduce the risk of colonic malignancy in this setting.
HEPATOBILIARY MALIGNANCIES AND GALLBLADDER DISEASE

Cholangiocarcinoma and Hepatocellular Carcinoma
Patients with PSC are prone to develop a variety of hepatobiliary malignancies (110, 111). The most important is cholangiocarcinoma; the risk of this is several hundred times higher in patients with PSC when compared with patients without PSC (94). Smoking and alcohol abuse have been suggested by some to increase the risk, but this has not been consistently demonstrated. Nevertherless, these patients should avoid smoking and alcohol abuse. The diagnosis of cholangiocarcinoma can be challenging. The 10-year cumulative risk is around 8% (85). Clear-cut risk factors for the development of cholangiocarcinoma in the setting of PSC are not known. Hepatocellular cancers have been described in some series, but hepatocellular cancer complicating PSC appears to occur quite infrequently (112, 113). Another study has suggested that patients with PSC may be prone to pancreatic cancers, but this study has not been confirmed (114, 115).
The differentiation of cholangiocarcinoma from a benign stricture arising a setting of PSC is difficult. CA 19-9 levels have been used and may be of value, although there are a number of patients with high CA 19-9 levels with no evidence of cholangiocarcinoma, whereas there are a number of patients with normal or low levels, who do have an underlying cholangiocarinoma; therefore, CA, 19-9 has limited predictive value (115, 116, 117). Brush cytology is specific but quite insensitive. Sensitivity ranges from 18% to 40% from the literature and this has been improved by the use of FISH as discussed earlier (70, 118). FISH is of particular importance in this setting. The role of positron emission tomography scanning is problematic and controversial, and is not a widely adapted diagnostic tool (119, 120). Screening for cholangiocarcinoma with regular (every 6–12 months) cross-sectional imaging with ultrasound or MR and serial CA 19-9 measures is recommended by experts in this area, for all patients with PSC (107, 108).
Stones and Polyps
Patients with PSC have an increased risk of gallbladder cancer and gallstones themselves are found in a quarter of patients with PSC (109). The patients with PSC may also develop gallbladder polyps, and if these are >8 mm there is a risk of being or becoming malignant (121). At this point, cholecystectomy is typically recommended for lesions greater than >8 mm in diameter. It is recommended that surveillance of the gallbladder be done on at least an annual basis with ultrasound (109).
SPECIAL SITUATIONS

PSC-AIH Overlap Syndrome
PSC and autoimmune hepatitis may co-exist in the same patient and the prevalence of autoimmune hepatitis in patients with PSC is ˜10%, but has ranged from 1.4% to 17% in various studies of patients with PSC (1, 3). Patients with autoimmune hepatitis and PSC overlap syndrome tend to be younger than 25 years of age and have serum biochemical tests and autoantibodies suggestive of autoimmune hepatitis (1, 3). One study suggested that a large proportion of children with autoimmune hepatitis subsequently developed cholangiographic evidence of PSC (122).
Based on these data, it is reasonable to recommend that further testing for autoimmune hepatitis is appropriate among younger patients with PSC or those with higher-than-expected levels of aminotransferases usually >5 × the upper limit of normal. Similarly, it appears reasonable to recommend MRCP among younger patients (i.e., <25 years of age) with autoimmune hepatitis, who have elevated serum ALP usually >2 × the upper limit of normal (1).
PSC in Children
PSC appears to be much less common among children than adults, with an estimated prevalence 20% lower than in adults and is a rare indication for liver transplantation in this population (3). Furthermore, PSC in children is more often associated with higher serum aminotransferase levels and concomitant autoimmune hepatitis, and sclerosing cholangitis is a more common phenomenon, leading to the use of the term “autoimmune sclerosing cholangitis.” (1, 122) Serum ALP may be elevated in children due to bone growth; hence, suspected cholestasis should be confirmed by measurement of gamma-glutamyl transpeptidase levels. Cholangiocarcinoma appears to be rare in this population and surveillance for gallbladder cancer or cholangiocarcinoma is not recommended (3).
In summary, pediatric PSC may have a different clinical presentation than in adults and the workup should include efforts to identify concomitant autoimmune hepatitis, which may lead to a different therapeutic approach (i.e., corticosteroids or immunosuppressive medications). Current guidelines do not recommend routine surveillance for cholangiocarcinoma in children with PSC.
Immunoglobulin G4-Associated Cholangitis
IgG4-associated pancreatitis and cholangitis is being increasingly recognized in patients who present with sclerosing cholangitis. IgG4-associated autoimmune pancreatitis is a clearly described entity characterized by strictures in the pancreatic duct, elevated IgG4 levels and response to immunosuppressive therapy (reference). This condition may be associated with biliary strictures and elevated plasma IgG4 levels, and liver biopsy may reveal a lymphoplasmacytic infiltrate (1, 3). In some cases, the biliary disease is predominant and features of autoimmune pancreatitis may or may not be present. A subset of patients with PSC have marked elevations of IgG4 levels (>140 mg/dl), although mild increases in IgG4 levels appear common in PSC (40). Patients with IgG4-associated sclerosing cholangitis appears to be less likely to have IBD and there may be differences in cholangiographic appearance between PSC and IgG4 cholangitis (41). Corticosteroids or other immunosuppressive agents are generally used in patients with IgG4 cholangitis, whereas they do not have a role in PSC (1). Combination of predizone and azathioprine are used to treat autoimmune hepatitis and has been used by some.
Measurement of IgG4 levels is reasonable in patients with PSC and consideration should be given to imaging for autoimmune pancreatitis and the presence of IgG4-associated cholangitis among those with markedly elevated IgG4 levels. Liver biopsy should be considered to identify the classical lymphoplasmacytic infiltrate and consideration of immunosuppression therapy may be useful in such patients, especially if they have higher-than-expected elevations of serum aminotransferase levels.
GENERAL MANAGEMENT

Portal Hypertension
PSC causes progressive hepatic fibrosis and cirrhosis, which can lead to portal hypertension. The mechanisms of portal hypertension from PSC generally are not unique to this disease. Elevated portal pressure in cirrhosis is most commonly the result of increased resistance to portal blood flow combined with augmented portal inflow. Increased resistance to portal flow results from architectural distortion of the liver, associated with hepatic fibrosis and regenerative nodules. Evidence from rat models suggests that increased resistance to portal inflow may also result from active intrahepatic vasoconstriction due to decreased release of nitrous oxide (130). Portal venous inflow is increased in the rat model due to splanchnic vasodilation that is not adequately decompressed by porto-systemic collaterals (131).
In a small percentage of patients with PSC, portal hypertension may develop before cirrhosis due to pre-cirrhotic portal hypertension. Among 306 patients transplanted for PSC at 2 institutions, 11/306 (3.3%) patients had portal hypertension without cirrhosis due to nodular regenerative hyperplasia or obliterative venopathy (132). MELD exception points are not offered for patients with PSC and non-cirrhotic portal hypertension.
Complications of portal hypertension in PSC generally are not unique to this disease, and include gastroesophageal varices and variceal hemorrhage. Previous guidelines have addressed the management of gastroesophageal varices (133). Screening of patients with signs of advanced disease with platelet counts <150 × 103/dl is recommended (127).
However, patients with PSC and portal hypertension do sustain an increased rate of bleeding from peristomal varices. IBD associated with PSC may require proctocolectomy and peristomal varices develop in 25% of patients who have ileal stomas after colectomy (134). Peristomal varices can be avoided by ileal pouch–anal anastomosis in place of an ileal stoma. Hemorrhage from peristomal varices is treated effectively by decompression of the underlying portal hypertension with a transjugular intrahepatic portacaval shunt, portosystemic shunt surgery, or liver transplantation (135, 136, 137). Peristomal variceal hemorrhage may be treated by embolization of varices percutaneously or through balloon-occluded retrograde transvenous obliteration, as described in case reports (138, 139).
FAT-Soluble Vitamin Deficiencies
Fat-soluble vitamin deficiencies can occur in late stages of PSC when patient becomes jaundiced. Levels of vitamins A, E, and D should be assessed in patients with advanced disease (129).
Pruritus
Pruritus in patients with PSC is similar to that in other cholestatic liver diseases. It is often worse at night, in warm, humid climates, and may lead to excoriations from scratching, as well as other dermatologic complications (123). Pruritus may have a negative impact on quality of life and sometimes lead to suicidal ideation; pruritus may rarely be considered an indication for liver transplantation (140). In patients with PSC, who have a cholestatic pattern of liver test abnormalities, pruritus can generally be ascribed to cholestasis and empiric treatment is appropriate.
The management of pruritus should be directed to the underlying cause of cholestasis. In PSC, therapeutic intervention for patients with a dominant stricture should be considered. Medical management of pruritus is directed by the severity of the underlying pruritus. Mild pruritus may be treated with skin emollients and possibly antihistamines. More severe pruritus is best managed by bile acid sequestrants, such as cholestyramine. A total daily dose of cholestyramine of 4–16 g is needed to maintain symptom control (124). Second-line therapies include rifampin, at a dose of 150–300 mg twice daily (liver tests and serum bilirubin should be monitored during rifampin therapy to evaluate for hepatotoxicity), naltrexone (up to 50 mg/day), sertraline (75–100 mg per day) or phenobarbital (90 mg at bedtime) (125, 126).
Metabolic Bone Disease
Metabolic bone disease is a common complication of chronic liver disease, especially with chronic cholestasis. Osteoporosis has been reported in 13%–60% of patients with cholestatic liver disease (141). BMD in PSC is significantly lower than expected for age-matched controls (142). In a cohort of 237 patients monitored by serial BMD measurements over the course of 10 years, osteoporosis was diagnosed in 36/237 (15%) and osteopenia was found in 41% (128). The risk of osteoporosis increased with greater age, low body mass index, and longstanding IBD; three quarters of patients with all three of these risk factors had osteoporosis. Those patients with PSC, who underwent liver transplantation, have an additional risk of bone disease due to inactivity and dietary limitations, with a resultant increased risk of bone fractures and avascular necrosis (143).
The pathophysiology of bone disease in cholestatic liver disease is not known, and most studies have focused specifically on metabolic bone disorders in primary biliary cirrhosis rather than PSC. With these caveats, it is recognized that cholestatic liver disease predisposes to osteopenia and osteoporosis, which is associated with decreased bone formation, but there is not an increased risk of osteomalacia (144). Supplemental vitamin D and calcium has not been shown to reduce the risk of metabolic bone disease in this group of patients (145). The mechanism of decreased bone formation in cholestasis is uncertain. In theory, retained toxins from inadequate biliary excretion may predispose to bone disease, but treatment with UDCA has not offered benefit (146, 147).
Metabolic bone disease is diagnosed by low BMD as compared with age-matched controls. Dual-energy X-ray bone absorptiometry is applied to the lumbar vertebrae and femoral neck to measure BMD. By the World Health Organization scale, a BMD t-score of < −2.5 is diagnostic of osteoporosis and a t-score < −1.0 is diagnostic of osteopenia (negative t-scores indicate the number of s.d. below normal for age-matched controls) (148). The risk of fractures increases progressively with the decrease in t-scores: a decrease in t-score by one indicates a two- to threefold increased risk of fracture.
Treatment of metabolic bone disease in PSC is comparable to treatment for osteopenia and osteoporosis of any cause. Patients are advised to undergo weight-bearing exercise and take calcium and vitamin D supplementation. BMD is performed at diagnosis and every 2–4 years thereafter. The role of bisphosphonates for treatment of osteoporosis in PSC is not proven. However, in patients with osteopenia and primary biliary cirrhosis, alendronate treatment has resulted in significant improvement in BMD, both at the lumbar spine and the femoral neck, suggesting that alendronate may be useful for treatment of osteopenia and osteoporosis in patients with PSC (149).
SUMMARY OF RECOMMENDATIONS
- MRCP is preferred over ERCP to establish a diagnosis of PSC. (Strong recommendation, moderate quality of evidence) (4, 5, 20)
- Liver biopsy is not necessary to make a diagnosis in patients with suspected PSC based on diagnostic cholangiographics findings. (Conditional recommendation, low quality of evidence) (21)
- Liver biopsy is recommended to make a diagnosis in patients with suspected small duct PSC or to exclude other conditions such as suspected overlap with autoimmune hepatitis. (Conditional recommendation, moderate quality of evidence)(22, 23, 24)
- Antimitochondrial autoantibody testing can help exclude primary biliary cirrhosis. (Conditional recommendation, moderate quality of evidence) (25)
- Patients with PSC should be tested at least once for elevated serum IgG4 levels. (Conditional recommendation, moderate quality of evidence) (26, 27, 28)
- UDCA in doses >28 mg/kg/day should not be used for management of patients with PSC. (Strong recommendation, high quality of evidence) (42)
- ERCP with balloon dilatation is recommended for PSC patients with dominant stricture and pruritus, and/or cholangitis, to relieve symptoms. (Strong recommendation, low quality of evidence) (64, 65, 66, 67, 68)
- PSC with a dominant stricture seen on imaging should have an ERCP with cytology, biopsies and FISH to exclude diagnosis of cholangiocarcinoma. (Strong recommendation, low quality of evidence) (69, 70)
- PSC patients undergoing ERCP should have antibiotic prophylaxis to prevent post-ERCP cholangitis. (Conditional recommendation, low quality of evidence) (71)
- Routine stenting after dilation of a dominant stricture is not required, whereas short-term stenting may be required in patients with severe stricture. (Conditional recommendation, low quality of evidence) (68, 72)
- Liver transplantation, when possible, is recommended over medical therapy or surgical drainage in PSC patients with decompensated cirrhosis, to prolong survival. (Strong recommendation, moderate quality of evidence) (94, 95, 96)
- Patients should be referred for liver transplantation when their MELD score exceeds 14. (Conditional recommendation, moderate quality of evidence) (97)
- Annual colon surveillance preferably with chromoendoscopy is recommended in PSC patients with colitis beginning at the time of PSC diagnosis. (Conditional recommendation, moderate quality of evidence) (104)
- A full colonoscopy with biopsies is recommended in patients with PSC regardless of the presence of symptoms to assess for associated colitis at the time of PSC diagnosis. (Conditional recommendation, moderate quality of evidence) (3)
- Some advocate repeating the exam every 3–5 years in those without prior evidence of colitis. (Weak recommendation, low quality of evidence) (3)
- Consider screening for cholangiocarcinoma with regular cross-sectional imaging with ultrasound or MR and serial CA 19-9 every 6–12 months. (Conditional recommendation, very low quality of evidence) (107, 108)
- Cholecystectomy should be performed for patients with PSC and gallbladder polyps >8 mm, to prevent the development of gallbladder adenocarcinoma. (Conditional recommendation, very low quality of evidence) (109)
- Further testing for autoimmune hepatitis is recommended for patients <25 years of age with PSC or those with higher-than-expected levels of aminotransferases usually 5 × upper limit of normal. (Conditional recommendation, moderate quality of evidence) (1, 3)
- MRCP is recommended for patients <25 years of age with autoimmune hepatitis, who have elevated serum ALP usually >2 × the upper limit of normal. (Conditional recommendation, moderate quality of evidence) (1)
- Local skin treatment should be performed with emollients and/or antihistamines in patients with PSC and mild pruritus, to reduce symptoms. (Conditional recommendation, very low quality of evidence) (123, 124)
- Bile acid sequestrants such as cholestyramine should be taken (prescribed) in patients with PSC and moderate pruritus, to reduce symptoms. Second-line treatment such as rifampin and naltrexone can be considered if cholestyramine is ineffective or poorly tolerated. (Conditional recommendation, very low quality of evidence) (124, 125, 126)
- Recommend screening for varices in patients with signs of advanced disease with platelet counts <150 × 103/dl. (Conditional recommendation, very low quality of evidence) (127)
- Patients with PSC should undergo BMD screening at diagnosis with dual energy X-ray absorption at diagnosis and repeated at 2- to 4-year intervals. (Conditional recommendation, moderate quality of evidence) (128)
- Patients with advanced liver disease should be screened and monitored for fat-soluble vitamin deficiencies. (Conditional recommendation, moderate quality of evidence) (129)
ACKNOWLEDGMENTS
This guideline was produced in collaboration with the Practice Parameters Committee of the American College of Gastroenterology. The Committee gives special thanks to Rishi Pawa, MD, who served as guideline monitor for this document.
REFERENCES