ACG Clinical Guideline: Epidemiology, Risk Factors, Patterns… : Official journal of the American College of Gastroenterology

INTRODUCTION
This clinical guideline was designed to address colon ischemia (CI) including its definition, epidemiology, risk factors, presentations, methods of diagnosis, and therapeutic interventions. Each section of the document will present key recommendations or summary statements followed by a comprehensive summary of supporting evidence. An overall summary of all recommendations is listed in Table 1.

Recommendations and summary statements

Continued.
A search of MEDLINE (1946 to present) and EMBASE (1980 to present) with language restriction to English was conducted using the search terms ischemic colitis, ischaemic colitis, colon ischemia, colonic ischemia, colon ischaemia, colonic ischaemia, colon gangrene, colonic gangrene, colon infarction, colonic infarction, rectal ischemia, rectal ischaemia, ischemic proctitis, ischaemic proctitis, cecal ischemia, cecal ischaemia, ischemic colon stricture, ischaemic colon stricture, ischemic colonic stricture, ischaemic colonic stricture, ischemic megacolon, ischaemic megacolon, colon cast, and colonic cast. The references obtained were reviewed and the best studies were included as evidence for guideline statements or in the absence of quality evidence, expert opinion was offered.
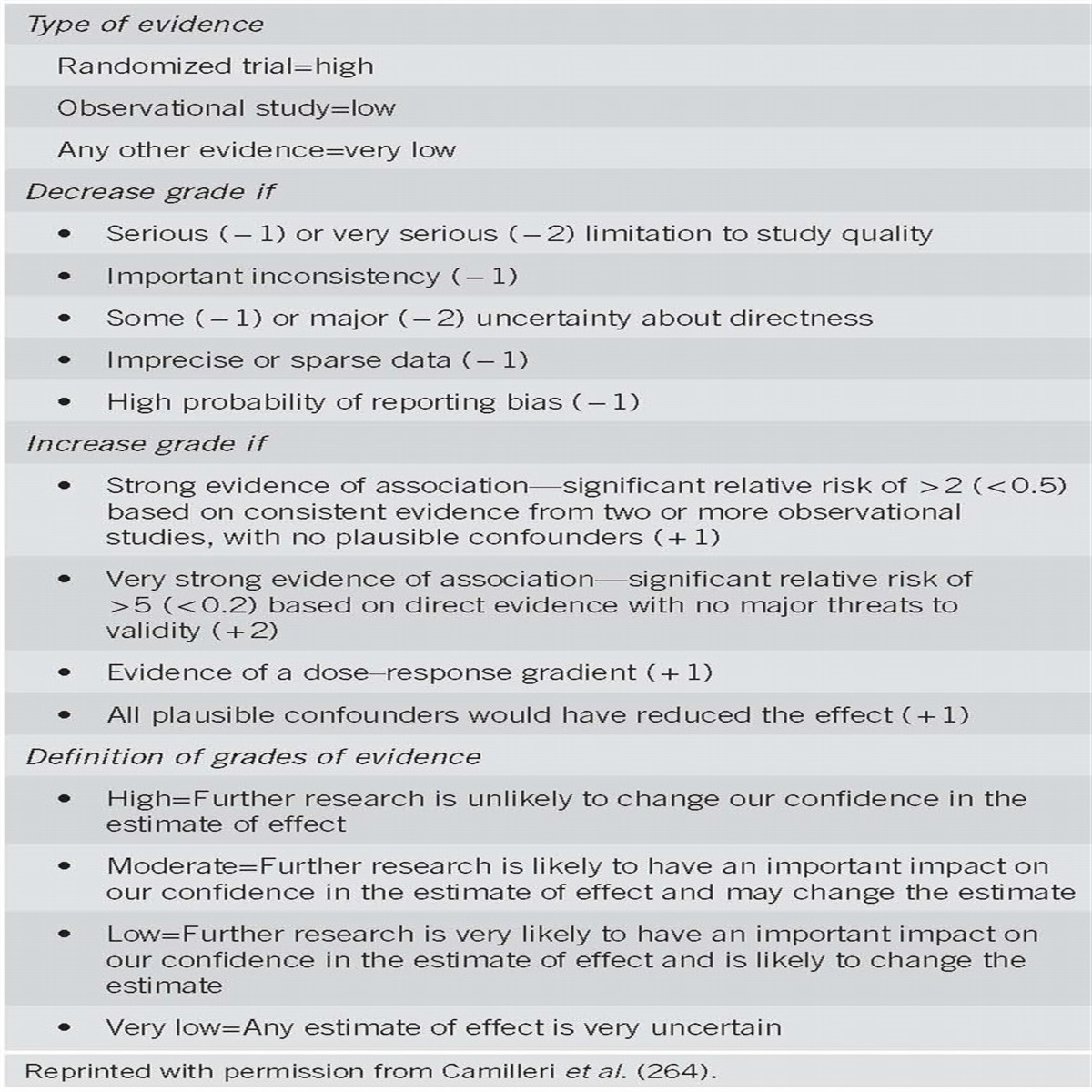
The GRADE system (Grading of Recommendations Assessment, Development, and Evaluation) was used to evaluate the quality of evidence and strength of recommendations (1, 2). The level of evidence ranged from “high” (implying that further research was unlikely to change the authors’ confidence in the estimate of the effect) to “moderate” (further research would be likely to have an impact on the authors’ confidence in the estimate of effect) to “low” (further research would be expected to have an important impact on the authors’ confidence in the estimate of the effect and would be likely to change the estimate) to “very low” (any estimate of effect is very uncertain). The strength of a recommendation was graded as “strong” when the desirable effects of an intervention clearly outweighed the undesirable effects and as “conditional” when there was uncertainty about the tradeoffs between the desirable and undesirable effects of an intervention. Of note, in this clinical guideline there are several sections focusing on factors associated with prognosis in CI. Because the GRADE system currently is not designed to rate the quality of the literature for these topics, we have preceded each of these sections with “summary statements” that detail the most important concepts regarding each area, but without a GRADE rating.
DEFINITION
CI is the condition that results when blood flow to the colon is reduced to a level insufficient to maintain cellular metabolic function. The end result of this process is that colonocytes become acidotic, dysfunctional, lose their integrity and, ultimately, die. Although the etymologic root of the word ischemia is from the Greek iskhaimos, meaning a “stopping of the blood,” we now know that blood flow need not stop but only diminish significantly to cause ischemic damage. Moreover, ischemia may be followed by reperfusion injury and, for relatively brief periods of ischemia, this combined injury may produce more damage than just reduction of blood flow without reperfusion. The degree to which colonic blood flow must diminish before ischemia results varies with the acuteness of the event, the degree of preexisting vascular collateralization, and the length of time the low flow state persists. CI may manifest with reversible or irreversible damage. Reversible damage includes colopathy, i.e., subepithelial hemorrhage or edema, and colitis; colitis reflects an evolutionary stage in which the overlying mucosa ulcerates as the subepithelial edema and blood are resorbed. In reversible disease, such resorption occurs rather promptly, usually within 3 days. Ulcerations may persist for several months before resolving, although during this time, the patient usually is asymptomatic. Irreversible manifestations of CI include gangrene, fulminant colitis, stricture formation, and, rarely, chronic ischemic colitis. Recurrent sepsis due to bacterial translocation is another rare manifestation of irreversibly damaged bowel.
EPIDEMIOLOGY
The absence of a unique diagnosis code for acute large bowel ischemia in the ICD-9-CM (International Classification of Diseases, 9th Revision, Clinical Modification) challenges case finding for research. This system, which is commonly used in the United States, assigns the hospital discharge code 557.0 (acute vascular insufficiency of intestine) and 557.9 (unspecified vascular insufficiency of intestine) to ischemic colitis as well as many other small and large bowel entities. This limitation persists in the newer ICD-10-CM classification system. Therefore, either medical records must be reviewed carefully or clear stipulations must be applied to databases to reliably identify patients with CI (3).
CI, the term we prefer to ischemic colitis because some patients do not have a documented inflammatory phase of disease, is the etiology in 9–24% of all patients hospitalized for acute lower gastrointestinal bleeding (4, 5, 6), ranking CI first (5), second (4, 7), or third (6) behind colorectal malignancy in large epidemiological surveys. A national insurance claims-based survey of patients hospitalized with CI revealed an annual incidence rate of 17.7 cases/100,000 (8). In the population-based, record-review study of patients hospitalized in the Kaiser San Diego Medical Care Program, the estimated annual incidence was 15.6 patients/100,000 (women, 22.6; men, 8.0) (9). Because of multiple admissions of some patients, the hospitalization rate was 16.4/100,000 per year with 6% of episodes developing after hospitalization for surgery or medical treatment of another disease. A recently published population-based study yielded an incidence of 16.3 cases/100,000 person-years with a nearly fourfold increase over 34 years (10).
Children with CI are only rarely reported (11, 12), but CI occurs in adults of all ages and increases with age, especially after age 49 years (8, 9). An insurance claims-based study reported an incidence of only 7.2 cases/100,000 person-years (13), although few people of at least 60 years of age were surveyed, possibly explaining this relatively low incidence. CI is more common in women than in men, and 57–76% of patients in large series have been female (8, 9, 10, 14, 15, 16, 17, 18). One survey found that female predominance was especially great after age 69 years and that most patients <50 years old and all patients <40 years old were women (9). There seems to be much less female predominance among young Japanese patients (19).
Mortality rates in large series range from 4 to 12%, but inclusion criteria, case ascertainment methods, and rates of comorbidity and surgery in these studies differed (7, 9, 10, 17, 18, 20). Recurrent CI increases over time; for example, estimated cumulative recurrence rates at 1, 2–3, 4, and 5–6 years were 3%, 5%, 6%, and 10%, respectively, in one study (9) and 3.3% at 2 years and 7.5% at 5 years in another study (10). Particular predisposing illnesses have been reported with recurrent disease, such as hypercoagulable states (21). Therefore, in any large survey, recurrence will be related to the relative proportions of patients with spontaneous, idiopathic disease and those with illnesses likely to foster recurrence.
PATHOPHYSIOLOGY
CI can result from alterations in the systemic circulation or from anatomic or functional changes in the mesenteric vasculature; the proximate cause is thought to be local hypoperfusion and reperfusion injury. In most cases, no specific cause for ischemia is identified, and such episodes are attributed to localized nonocclusive ischemia, likely a result of small-vessel disease. These patients are sometimes classified as having Type I disease. By contrast, in Type II disease the etiology is identified and most commonly follows an episode of systemic hypotension, decreased cardiac output, or aortic surgery (22). This classification schema for CI is infrequently used in clinical settings, but in practice, patients with Type II disease can have therapy targeted toward the underlying cause, whereas Type I CI is treated in a broader and supportive manner. An increasing variety of causes of CI is being defined (see “Risk Factors” section).
Abnormalities seen on angiography rarely correlate with clinical manifestations of CI, and age-related abnormalities in the splanchnic vessels are not uncommon, including narrowing of small vessels, and tortuosity of the long colic arteries; fibromuscular dysplasia of the superior rectal artery has been associated with CI. The colon is particularly susceptible to ischemia, perhaps owing to its relatively low blood flow, its unique decrease in blood flow during periods of functional activity, and its sensitivity to autonomic stimulation. What triggers the episode of CI, however, usually is not identified.
RISK FACTORS
Summary statements
- Comorbid cardiovascular disease and diabetes mellitus should increase consideration of CI in patients with typical clinical features (10, 14, 15, 20).
- A history of irritable bowel syndrome (IBS) and constipation should be sought in patients suspected to have CI (8, 13, 15).
- Selective cardiology consultation is justified in patients with CI, particularly if a cardiac source of embolism is suspected (23).
- Chronic kidney disease and chronic obstructive pulmonary disease are associated with increased mortality from CI (7, 10, 24, 25).
- Evaluation for thrombophilia should be considered in young patients with CI and in all patients with recurrent CI (26, 27, 28).
- Surgical procedures in which the inferior mesenteric artery (IMA) has been sacrificed, such as abdominal aortic aneurysm repair and other abdominal operations, should increase consideration of CI in patients with typical clinical features (14, 29, 30).
- In patients suspected of having CI, a history of medication and drug use should be sought, especially constipation-inducing medications, immunomodulators, and illicit drugs (9, 15, 31).
Summary of evidence
Five large case–control studies of risk factors for CI examined both associated medical conditions and drug use (10, 14, 15, 20, 32), and three of them also assessed surgical history (10, 14, 15). The multivariate analyses used in these studies considered potential risk factors together rather than only individually to detect those that imposed a risk independent of the influences of other variables. Comparisons of these studies thus must be viewed in light of the variations in factors assessed and other differences in research methods. Table 2 displays the entities for which the data seem most rigorous in view of research methods and consistency of findings across studies. Study limitations are inclusion of relatively few elderly patients (14), reliance on medical claims data without comprehensive record review (14, 15), reliance on recorded use of drugs rather than billing or dispensing records (10), and uncertain accuracy of diagnoses assessed from ICD-9-CM codes, especially disorders identified by symptoms only, such as diarrhea (32), constipation (15), and IBS (14, 15, 32). Because some studies did not exclude certain symptoms and entities coded during a short period before the index date of CI, the authors could have erred by attributing risk factor status to coded variables that mimicked or shared acute features of CI, including bloating (15), dyspepsia (15), dysentery (15), rectal bleeding (14), IBS (14, 15), nonspecific colitis (14), and use of antidiarrheal drugs (14) and histamine type 2 receptor antagonists (15). There are statistical limits on the analysis of potentially important drugs (33) that have low frequency of use (e.g., chemotherapeutic agents or phentermine) or are absent from controls (32). Moreover, all studies are limited in analyzing some over-the-counter drugs, e.g., pseudoephedrine, some laxatives, nonsteroidal anti-inflammatory drugs, as well as illicit drugs (33), because pharmacy dispensing data do not comprehensively capture use and patient history may be inaccurate. Ascertainment bias also could result in increased detection of CI in patients with a disorder such as IBS who likely undergo colonoscopy more often than controls (34). Finally, it is important to understand that statistical association does not equal causality.

Medical conditions and surgical history independently associated with colon ischemia in multivariate analyses of case–control studies
Medical conditions
Cardiovascular and pulmonary risk factors for CI are reflected by the comorbidities reported in six series totaling 1,955 patients (7, 9, 10, 17, 18, 20): hypertension (57–72%), diabetes mellitus (17–28%), coronary artery disease (18–37%), dyslipidemia (18–33%), chronic obstructive pulmonary disease (10–18%), congestive heart failure (9–16%), atrial fibrillation (9–14%), peripheral vascular disease (8–21%), and renal disease (4–18%). CI also has accompanied type IIIb aortic dissection (35). Coronary artery disease and atrial fibrillation were approximately twice as common in patients with isolated right-colon ischemia (IRCI) compared with other anatomic patterns of CI that are generally less severe (7). Using electrocardiography, Holter monitoring, and transthoracic echocardiography in patients with CI, a French group found a “proven” potential cardiac source of embolism in 35% of patients, primarily those with sustained or paroxysmal atrial fibrillation (36). Although they recommended doing all of these tests routinely, many of the patients had abnormalities that could be detected by physical examination. Nonetheless, selective diagnostic evaluation and cardiology consultation seems justified. CI occurred within 3 days of acute myocardial infarction in 0.13% of patients, and complications and mortality were higher in patients with both diseases than in those with either CI or myocardial infarction alone (37). Among patients with severe hematochezia, patients with CI more often had moderate or severe lung disease than did patients with other colonic causes of hemorrhage (38), and chronic obstructive pulmonary disease independently predicted mortality in series from Montefiore Medical Center in New York and the Mayo Clinic in Rochester, Minnesota (7, 10).
Hypertension and diabetes mellitus independently predicted CI among patients with acute lower abdominal pain (39). Endothelial dysfunction could contribute to the effects of hypertension (40) and diabetes (41) and has been offered to explain the increased risk of CI associated with rheumatic autoimmune diseases (42), including rheumatoid arthritis (43), although association of hypercoagulable states with these diseases is another potential risk factor (21, 43, 44, 45).
Interest in IBS as a potential risk factor for CI arose after alosetron hydrochloride, used to treat women with diarrhea-predominant IBS, was withdrawn from the US market because of reports of CI among alosetron users during the first few months after its release in 2000. In a medical claims-based study of subjects mainly <60 years of age, Cole et al. (13) found the incidence of CI was 3.4 times greater in patients with IBS than those without IBS. In another study, the relative risk for CI was 3.2 and 2.8 times higher for those with IBS and constipation, respectively, than for those who lacked these disorders (8). Subsequently, four case–control studies applied more extensive multivariate analysis to the assessment of IBS as a risk factor for CI; three studies confirmed it did convey increased risk (14, 15, 32), including one study that found an association in women only (32), and the fourth one found no statistically significant risk (10). Excessive sympathetic activity in IBS (46) could impair vasodilation in the mesenteric vessels, the most reactive vascular bed in the body (47). A retrospective review found that physicians recorded constipation immediately preceding the presenting features of CI in only 7% of patients (9), but a prospective study detected constipation during the 30 days before presentation in 25% of cases (17). Constipation could mediate increased risk through increased intracolonic pressure and reduced blood flow (48) as a result of fecal impaction, and constipation preceding the symptoms of CI could be a clinical clue for differential diagnosis. Diarrhea was a risk factor in one study (32) but, as with constipation (15), CI could have been a diagnosis applied to patients with IBS.
Renal disease has also been described as a risk factor for CI from observational studies, but it has not been identified as an independent predictor in case–control studies. In one survey, absence of dialysis dependency in controls prevented its inclusion in multivariate analysis (32). However, severe chronic kidney disease was present in 11% of cases from Montefiore Medical Center and was nearly 3 times as common in patients with IRCI as other cases in that series (7), similar to the findings of Taiwanese (24) and Korean (49) studies. Thus, 7% of cases of CI reported by Paterno et al. (18) were dialysis dependent; 33% of the cases described by Flobert et al. (25) required hemodialysis, and right-sided disease occurred in 3 times as many patients on hemodialysis than in other patients. The most obvious causative link, although unproven, in patients on dialysis in whom CI (predominantly IRCI) develops is fluctuation in fluid balance with a decrease in circulating blood volume. Among patients with severe hematochezia, the mean serum creatinine was twice as high in patients with CI as it was in those with other colonic causes (38), and hemodialysis independently predicted CI in patients with acute lower abdominal pain (39).
Thrombophilia is another potential risk factor for CI. There are numerous case reports of various coagulopathies in patients with CI, including deficiencies of protein C, protein S, antithrombin III, and factor V Leiden mutation (21, 45, 50). In particular, the “catastrophic” variant of the antiphospholipid syndrome causes multiple vascular occlusions, especially in small vessels, but typically causes more widespread intestinal ischemia than CI alone (44). Thrombophilic abnormalities were described in 72% of frozen blood samples of ambulatory patients from Crete (26) and in 28% of US patients’ blood drawn at least 1 month after the diagnosis of CI (27). Furthermore, genetic polymorphisms associated with thrombophilia and vascular hyperactivity were found in more young patients with CI than in controls (28). Concerns about attributing an etiologic role to these findings include uncertainty regarding whether the clotting abnormalities actually contributed to CI or were epiphenomena of little significance. For example, it is difficult to reconcile a major etiologic role for coagulopathy in view of the advanced age of many CI patients and the low recurrence rate of CI. In one study, 14% of patients with CI had reduced levels of free protein S (26) that can occur as a result of its binding to an acute-phase reactant. Eight per cent of healthy controls had reduced levels of protein S, and 4% had reduced antithrombin, activated protein C resistance, or a factor V Leiden mutation, raising concerns about the assays or study population (51). At this time, routine testing for a coagulation disorder in most patients with CI does not appear justified, although it seems reasonable in young patients with CI and in patients with recurrent disease (21).
At least a dozen cases of CI have been reported following long-distance running in runners who were 26-42 years of age, most of whom were women. CI involved the right colon in 10 patients and extended to the left side in 3 of them; in 2 patients CI was limited to the left colon. Two patients underwent resection of the ischemic segment, and both survived. Young age, a female predominance, and lack of mortality contrast with usual series of IRCI (52, 53, 54, 55). Ischemia is a postulated cause of diarrhea, abdominal pain, hematochezia, and occult bleeding in endurance athletes (55, 56, 57).
Sickle cell crisis with microvascular occlusion can also cause CI. Of the 7 reported cases, patients were 5–35 years of age and the distribution varied from sigmoid to pancolonic; 3 patients underwent colon resection and 2 died (58, 59, 60, 61). Two reported cases of CI occurred in patients with sickle cell trait: a 44-year-old woman with diastolic dysfunction survived two episodes of CI of undocumented distribution (62), and a 52-year-old woman who also had Sjogren’s disease survived sigmoid CI (63). Sickle cell disease is only rarely mentioned as an etiology for CI, but the rate of this disease causing CI could be higher in populations with a greater proportion of patients who are of African ancestry (9).
CI has also rarely followed colonoscopy (64, 65, 66, 67, 68); such reports include one patient who had other predisposing features (68). Postcolonoscopy CI could result from reduced colonic blood flow as a consequence of luminal distention and increased intraluminal pressure, both of which are more pronounced with insufflation by air than by carbon dioxide (69). There have been various other associations with CI including carbon monoxide poisoning (70), pheochromocytoma (71), air embolism after deep-sea diving (72), colon carcinoma (73), and, after airplane flights (74), a pit viper bite (75), blunt trauma to the abdomen (76), and repetitive jackhammer trauma (77).
Surgical history
A survey of 89,967 admissions for abdominal aortic aneurysm (AAA) repair revealed an overall rate of postoperative CI of 2.2%: with repair of ruptured AAA, 8.9%; with open elective AAA repair, 1.9%; and with endovascular AAA repair, 0.5% (29). Routine postoperative sigmoidoscopy after AAA repair reveals that mild CI occurs much more often than does symptomatic CI (30). Repair of AAA had preceded CI in only <1–2% of all cases of CI in reported series (7, 9, 20). A major mechanism for CI after these vascular procedures is sacrifice of the IMA. One study identified prior laparoscopy as a risk (with a wide confidence interval) but did not specify the surgery performed (odds ratio 17.67, 95% confidence interval 1.91–163.57) (15). Ligation of the IMA could also explain CI in patients who have undergone surgery for colon carcinoma (78, 79).
Drug use
When drug-induced CI was reviewed in 2007, there was evidence to propose various major classes of pharmacologic agents as predisposing to CI (33). Additional publications have since provided more evidence for the pathogenic role of certain drugs, taking into account reported single cases and other publications, including case–control studies, We believe that constipation-inducing drugs, immunomodulators, and illicit drugs are best supported as etiologic agents, but there is some support for a role of many disparate drug classes (Table 3).

Drugs proposed to predispose to CI, estimate of evidence level, and postulated pathogenesis

Continued.
Despite extensive observations on the above clinical factors associated with CI, there are no specific identifiable risk factors for CI in most patients, and some patients have multiple risk factors. The heterogeneous risk factors for CI support its multifactorial pathogenesis and indicate the importance of careful assessment of the medical, surgical, and drug use history in every patient with CI. Further research into the cause of CI and its risk factors is needed.
CLINICAL PRESENTATION
Recommendations
- The diagnosis of CI is usually established because of symptoms including sudden cramping, mild, abdominal pain; an urgent desire to defecate; and passage within 24 h of bright red or maroon blood per rectum or bloody diarrhea (7, 9, 17) (strong recommendation, very low level of evidence).
- A diagnosis of non-IRCI should be considered when patients present with hematochezia (strong recommendation, very low level of evidence) (7, 9, 17).
Summary statement
- CI isolated to the right colon (IRCI) is associated with higher mortality rates compared with other patterns of CI (7, 17).
Summary of evidence
CI generally manifests with sudden cramping, mild, left lower abdominal pain; an urgent desire to defecate; and passage within 24 h of bright red or maroon blood per rectum or bloody diarrhea (7, 9, 80, 81). Longstreth and Yao (9) reported a large retrospective study of 401 patients admitted with CI in which the most common symptoms of presentation were abdominal pain (87%), rectal bleeding (84%), diarrhea (56%), and nausea (30%). A separate analysis of 72 Canadian patients with biopsy-proven CI showed that abdominal pain (77.8%), hematochezia (58.3%), bloody diarrhea (34.7%), and nonbloody diarrhea (19.4%) were among the most common presenting features (80). Abdominal pain, urgent need to defecate, and bloody diarrhea are the major features, and all three symptoms occur in this temporal sequence in nearly one-half of cases (17); vomiting (30%), dizziness (10%), and syncope (6%) occur less frequently (9). Pain typically precedes bleeding and is usually mild to moderate, although robust systematic assessment of its severity has not been performed to date (17). Abdominal tenderness is usually present over the involved segment of colon. Notably, patients with IRCI more commonly have pain than they do rectal bleeding; only 25–46% of patients with IRCI have rectal bleeding, and physicians should entertain the diagnosis of IRCI for patients with acute, severe abdominal pain who lack hematochezia and/or diarrhea, especially if they have the clinical scenarios associated with IRCI, such as dialysis, sepsis, and hypotension or shock (9, 16, 17).
The duration of symptoms is difficult to quantify in patients with CI given the often mild and benign course of disease. One study from Switzerland looked at the time to presentation for a cohort of 49 patients with biopsy-proven CI: 57.1% presented within 24 h of symptom onset and 75.5% within 3 days of symptoms (81). In more than half of the cases of CI, the disease is reversible. Symptoms of CI generally resolve within 2–3 days and the colon heals in 1–2 weeks. With severe injury, it may take up to 6 months for the colon to heal; however, during this time the patient is usually asymptomatic.
Rectal bleeding is usually mild in CI, but in one retrospective analysis of 550 patients presenting with severe hematochezia, 11.8% were found to have CI as the cause (38). Severe bleeding was seen more frequently in women and in patients with severe lung disease, elevated creatinine and glucose levels, and those on anticoagulation. The 30-day outcomes for rebleeding, surgical intervention, and mean number of hospital days were worse for those with CI compared with other etiologies of lower gastrointestinal bleeding (38). Severe hemorrhage occurs mainly in patients with gangrenous CI, fulminant pancolitis, and IRCI (17). Montoro et al. (17) reported that 42.6% of their overall population of 364 patients with CI had a hemoglobin level of <12 g/dl, similar to the 36% rate of low hemoglobin in a more recent series (10). Blood transfusion is required in <5% of patients who present with CI (9, 17).
Most episodes of CI are benign and self-limited and only a minority of cases are severe. The study of Montoro et al. (17) found that gangrenous colitis and universal fulminant colitis are seen in 9.9% and 2.5% of cases, respectively. Symptoms that persist for more than 2 weeks are also associated with a higher incidence of acute complications and irreversible disease, such as gangrene and perforation, segmental ulcerating colitis, or stricture. Symptoms of patients with severe disease do not necessarily follow the classic sequence of abdominal pain, urgent desire to defecate, and bloody diarrhea. Indeed, less than one-third of patients from any of the groups of Montoro et al. (17) have classic symptom sequencing. Only the study of Montoro et al. (17) has rigorously assessed the characteristics of presentation of each of these clinical patterns and that report is used as a guide along with expert opinion for the clinical pattern presentations discussed below (17).
Anal passage of an infarcted colonic segment or “colonic cast” not accompanied by features of peritonitis is a rare complication of CI that has been described in the literature in 21 patients (82, 83, 84, 85). This complication usually occurs in patients with multiple medical comorbidities who recently underwent abdominal aortic aneurysm repair or colorectal surgery. All such cases of CI affected the left side of the colon and none have been reported that involve the right side despite the increasing incidence of right-sided ischemia. A cast of 25 to 120 cm in length is typically passed 2–4 weeks after the acute ischemic insult (82, 84, 85). Casts may consist of mucosa with or without submucosa or may be full thickness, in which case a tunnel of inflammatory tissue is left behind; the latter situation requires urgent surgical intervention.
Morphologic changes after CI vary with the duration and severity of the injury. The mildest injury is mucosal and submucosal hemorrhage and edema, with or without partial necrosis and ulceration of the mucosa. Iron-laden macrophages may be found and with more severe injury, submucosal fibrosis and pseudomembranes may develop. In 3.3–9.4% of cases, the muscularis propria is replaced by fibrous tissue forming a stricture, most of which are asymptomatic (80, 86, 87). Stricture formation is more common in patients with moderate CI, and was reported in 14.3% of cases; it was not seen in any patient with severe disease, because these patients were operated on promptly or had died (86). The quoted studies lack clear definitions of stricture, however, and these stricture rates are likely overestimates. Symptomatic strictures are rare, but further study is needed to define this frequency compared with that of silent stricture formation.
Acute severe CI can also mimic inflammatory bowel disease (IBD) with chronic ulcerations, crypt abscesses, and pseudopolyps (88). The most severe form of ischemic damage causes transmural infarction. Gangrenous colitis is characterized by increasing abdominal tenderness, guarding, rebound tenderness, rising temperature, and paralytic ileus. Abdominal pain is seen in the vast majority of these patients (86.1%) but rectal bleeding is far less frequent (30.6%); acute abdominal pain without rectal bleeding (58.3%) and nonbloody diarrhea (27.8%) are the most common clinical patterns of presentation (17).
Sudden onset of a toxic colitis with signs of peritonitis and a rapidly progressive course are typical of universal fulminant colitis, a rare variant of CI. The classic sequential triad is seen infrequently (11.1%) with this CI variant; symptoms of severe abdominal pain (66.7%) and rectal bleeding (55.6%) with abdominal tenderness on physical examination (85.9%) are the most characteristic presentation of universal fulminant colitis (17).
SEGMENTAL NATURE OF CI
Summary of evidence
The left colon is most commonly affected, but no colonic region is spared from involvement. In a large retrospective study of 313 patients, all of whom had their entire colon evaluated by colonoscopy, surgery, or autopsy—alone or in combination—and in all of whom CI was proven by biopsy, a segmental pattern was typical: the left colon was affected most often (32.6%), followed by the distal colon (24.6%), right colon (25.2%), and entire colon (7.3%) (7). In this study, although no specific etiology was associated with any specific anatomic distribution, pancolitis and IRCI were seen frequently in patients with sepsis, and IRCI was associated more frequently in patients with coronary artery disease and chronic kidney disease on hemodialysis (7). Similar results were found in large studies in California, Minnesota, and Spain (Table 4) (9, 10, 17). This pattern of involvement appears to be universal as a Korean cohort of 59 patients also showed a predominance of left-sided disease (64.1%) over right-sided involvement (35.9%) (49), although in this population, there were no differences between right- and left-sided CI in clinical characteristic presentations, cardiovascular risk factors, or the presence of diabetes mellitus; patients with IRCI, however, were more likely to have renal failure (49).

Segmental distribution of colon ischemia (CI)
The segmental nature of CI can be explained by the vascular anatomy of the colon and rectum. Colonic blood flow is supplied by three vessels: the superior mesenteric artery (SMA), IMA, and the superior hemorrhoidal artery. Vascular anatomy, however, is variable and often individually unique (89). Watershed areas of the colon are regions that are particularly susceptible to ischemic insult as a result of their location between two different vascular supplies. These areas include the splenic flexure (Griffith’s point) and sigmoid colon (Sudeck’s point). At the splenic flexure, there may be limited arcades (anastomotic artery, central collateral vessel, arc of Riolan) to link the left branch of the middle colic artery, which is a branch of the SMA, with the ascending branch of the left colic artery, which is derived from the IMA. Sudeck’s point refers to the last sigmoid arterial branch originating from the IMA, an area that has been thought to predispose the rectosigmoid to ischemic injury. The rectum is uncommonly affected by ischemia because of its relatively rich dual blood supply from both splanchnic and systemic arterial systems (90, 91, 92).
In older reports, certain causes were believed to affect particular segments: local nonocclusive ischemic injuries, the watershed areas; and ligation of the IMA, the sigmoid. Similarly, it has been said that the length of affected colon reflects the cause of CI, with atheromatous emboli involving short segments, and nonocclusive injuries involving longer portions of colon. These commonly quoted patterns of disease require further investigation to confirm their accuracy.
The segmental nature of CI has been known for decades, but only recently has it been shown that IRCI has a different clinical presentation and worse outcomes than CI affecting any other region of the colon (7, 16). As discussed earlier, patients with IRCI present most commonly with acute abdominal pain without rectal bleeding (59%) although when bleeding does occur it may be severe (17). Patients with IRCI have atrial fibrillation, coronary artery disease, and chronic kidney disease more frequently than do patients with CI affecting other areas of the colon (7, 49). Sotiriadis et al. (16) assessed 273 consecutive patients with biopsy-proven CI and found that compared with all other colon segments, IRCI had worse outcomes for 30-day mortality (22.5% vs. 11.9%, P=0.03), need for surgical intervention (54.9% vs. 10.9%, P<0.001), and unfavorable outcome (59.2% vs. 17.3%, P<0.001).These findings were reconfirmed in a more detailed follow-up study of 313 patients with pathologically confirmed CI, in which the 30-day mortality rate was 20.3% for IRCI compared with 9.0% in those with non-IRCI (P<0.01) (7). The poor outcome of IRCI has also been seen in several other studies. One showed an unfavorable outcome (mortality and/or colectomy) for IRCI of 40.9% compared with 10.3% for CI that involved the remainder of the colon (P<0.001), whereas another study had an unfavorable outcome of 33.6% for IRCI compared with 13.6% in isolated left segmental disease (P=0.02) (17, 49).
Isolated cecal necrosis was characterized in one case series of five patients presenting with acute abdominal pain, four of whom had peritoneal signs with either no changes in bowel habits or nonbloody diarrhea (22). Given the severity of symptoms, each patient was surgically explored with the clinicians’ differential diagnoses including cecal carcinoma or appendicitis. Eighty per cent of the patients had a history of cardiovascular disease or diabetes, although none had evidence of heart failure or myocardial infarction at the time of presentation and there was no identifiable etiology for the ischemic insult (22). Further study is required to clarify whether this rare segmental distribution of CI is a subdivision of IRCI with a similarly poor prognosis.
The pancolonic pattern of CI portends a similarly poor prognosis to that of IRCI. Brandt et al. (7) showed a mortality rate of 21.7% in patients whose entire colon was affected by CI. In this cohort, stage V chronic kidney disease (30.4%) and peripheral vascular disease (21.7%) were the most frequent comorbidities, and sepsis (70%) was the most common etiology. Longstreth and Yao (9) found that 61% of episodes of CI that required surgical intervention had either IRCI or bilateral (pancolonic) patterns of ischemia. The combination of these two disease distributions was associated with a hazard ratio of 14.6 (P<0.001) for CI that required surgery or led to death (9). When pancolonic involvement is observed, there probably was hypoperfusion in both the SMA and IMA circulations and the risk factors associated with such an episode likely forecast a worse outcome.
RECURRENT AND CHRONIC CI
Summary of evidence
Recurrence of CI is said to occur when a patient has one discrete episode that resolves and the patient subsequently re-presents with similar symptoms and has another independent diagnosis of CI. Defining the frequency and timing of recurrences is challenging, however, given the usually benign self-limited nature of CI and the fact that many patients with mild disease may not seek medical attention; there is also a lack of appropriate follow-up in the current literature. Studies that address long-term follow-up have significant variability in the time frames assessed, both among studies and within studies themselves. Some series with a 5-year follow-up have shown no recurrence (86, 93), whereas others detail recurrence rates of CI that range from 6.8 to 16.0% (9, 81, 94, 95). Huguier et al. (94) looked at a population of 73 patients who were admitted to a surgical service with CI and found that 6.8% of patients had had a recurrence of their CI with a mean follow-up of 4.5 years (range: 2–9 years). Of those who had recurrence, 80% of patients had a benign course and one patient had a fatal episode. Another study of 49 Swiss patients showed a recurrence rate of 16% with a median follow-up of 79 months (range: 6–163 months), but only 4.6% had biopsy-proven colonoscopic evidence of ischemia. This study found that, just as with the initial presentation, the most common symptoms of recurrence are abdominal pain, diarrhea, and hematochezia, although the frequency of these symptoms was not provided (81). 8.5% of 118 patients had recurrent disease during a 6-year follow-up in 2 community hospitals in Illinois. When comparing recurrent CI (70.6% pathologically confirmed) with nonrecurrent CI (80.6% histological confirmation), an abdominal aortic aneurysm (40.0% vs. 4.7%, P<0.01) and active smoking (50.0% vs. 18.7%, P<0.05) were more common in the recurrent cohort; no other significant differences in clinical presentation, CT scan findings, comorbidities, endoscopic features, or use of concomitant medications at the time of diagnosis were observed (95). A 16.7% recurrence rate was seen in a population of 72 Canadian patients with a mean follow-up of 9.5 months (range: 0–65 months); patients with coronary artery disease and elevated serum creatinine were 3.5- and 1.01-fold more likely to have a recurrence, respectively (80). The study of Longstreth and Yao of more than 400 patients detailed a recurrence rate of 10% at the 5–6-year follow-up period, noting that female gender and left-sided disease were more common in the recurrent population than in the population with only a single episode. In sum, although recurrence of CI does occur, it appears to be uncommon and the presentation and course seem to be the same as those of the initial episode; time to recurrence needs to be assessed further.
The question of whether CI can evolve into a chronic colitis remains controversial because of varying definitions of this potential entity. Chronic segmental colitis should be defined clinically by more than 3 months of typical symptoms and biopsy confirmation showing histologic evidence compatible with or characteristic of CI. The cases reported in the literature and presented below do not employ a uniform definition such as the one proposed above and, therefore, heterogeneity of this definition is seen among studies. The classic sequence of abdominal pain and urgent desire to defecate followed by bloody diarrhea (32.3%) is the most common presentation, although rectal bleeding without prior abdominal pains is also seen (30.8%) (17). Recurrent fever, leukocytosis, and septicemia suggest presence of an area of segmental colitis that is continually providing a portal of entry for colonic bacteria.
Estimates of the frequency of chronic ischemic colitis are variable and range from an unquantified “rare” to a controversially high rate of 25%, and are likely inaccurate (see below) (17). Montoro et al. (17) found that 17.9% of their population had chronic CI, but this study lacked stated criteria for diagnosis, leaving the frequency of occurrence in question. Other studies detail rates of up to 20–25%, but these estimates were made in an era predating colonoscopy, were based on barium enema findings, and likely overestimated recurrence rates. Pattern diagnosis without histologic confirmation would not meet the current rigors of modern diagnostic requirements (91).
It has been suggested by Wakefield and colleagues (96, 97, 98) that small multifocal gastrointestinal infarction and repetitive thrombotic mesenteric microvascular occlusion may play an etiologic role in IBD. A vascular etiology for IBD is supported further by studies showing that IBD occurs less frequently in patients with inherited disorders of coagulation (e.g., hemophilia or von Willebrand’s disease) and that smoking has a deleterious effect on the progression of Crohn’s disease (98, 99, 100). Almost 50 years ago, Boley first postulated that one or more bouts of CI might foster the development of chronic colitis via an autoimmune process. A study by Aroniadis et al. (101) of 18 patients with chronic CI showed that 71% of patients had at least one positive serum marker from a standard IBD diagnostic Prometheus panel. This finding in this rare subset of patients supports the concept of an autoimmune etiology for chronic CI. In a retrospective study published in 1981, Brandt et al. (102) studied 81 patients >50 years old who had new onset of symptoms of colitis and found that 75% of them had CI by a set of clinical, radiologic, and pathologic criteria and that one-half of these patients had been discharged with diagnoses of ulcerative, Crohn’s disease, or nonspecific colitis. A major weakness of this study, however, was its retrospective design and therefore the inability to exclude an infectious cause for the segmental chronic colitis in each case. In the same year, Reeders et al. (103) also described chronic CI but their study was flawed by including patients within 2 weeks of initial symptom onset and failure to provide information on the timing of development of chronic colitis compared with the time of initial diagnosis.
Longstreth and Yao (9) found no evidence of chronic colitis in their study of 401 patients. Some authors hypothesize that a chronic colitis might be the intervening process between an initial diagnosis of CI and the development of a stricture, but the studies that proposed this failed to characterize the intervening time when the chronic colitis might be evolving into a stricture. These studies additionally described the patients as asymptomatic during the intervening time interval and did not describe treatments of colitis before stricture development (86, 104, 105, 106). At this time, there are insufficient data to support chronic CI as a unique entity and further analysis is needed using a more uniform definition such as the one proposed earlier.
LABORATORY TESTING IN CI
Summary statements
- Laboratory testing should be considered to help predict CI severity (17, 94, 107).
- Decreased hemoglobin levels, low serum albumin, and the presence of metabolic acidosis can be used to predict severity of CI (17, 94, 107).
Summary of evidence
At this time, there is a shortage of well-controlled trials to assess the diagnostic and prognostic efficacy of laboratory tests in CI, but such testing is a useful tool to determine CI severity. Mosele et al. (107) retrospectively assessed laboratory values of 46 geriatric patients with biopsy-proven CI and compared the findings with an age-matched control group. They found that the mean serum white blood cell count (WBC, P<0.0001), creatinine (Cr, P=0.003), urea (P=0.008), and lactate dehydrogenase (LDH, P<0.0001) were higher in the CI group compared with the controls (107). The authors then compared severe disease (i.e., requiring surgical intervention or resulting in mortality) with mild disease (i.e., improving with conservative medical therapy) and found that only urea (14.5±8.9 vs. 8.2±5.3 mmol/l; P=0.02) and LDH (459±97 vs. 272±88.7 U/l; P=0.007) were higher in those with severe disease; there were no statistically significant differences in WBC or Cr (107). Montoro et al. (17) prospectively assessed 364 consecutive patients with definite or probable CI and found that WBC >15 × 109/l, hemoglobin (Hgb) <12 g/dl, and albumin <2.8 g/l were seen more frequently in patients with severe disease than in those with mild disease. By retrospectively analyzing 85 consecutive patients with CI, Añón et al. (108) found that those with severe disease had higher frequencies of anemia (Hgb <12 g/dl, 37.5% vs. 10.1%; P=0.012) and hyponatremia (serum sodium <136 mEql/l, 46.6% vs. 14.9%; P=0.012). One French study retrospectively evaluated 73 patients admitted to a surgical service with CI and showed that serum bicarbonate level <24 mmol was independently associated with severe CI (P=0.03); WBC >15,000/mm3 showed no significant association with disease severity (94). By comparing severe disease with mild disease, these studies sought to identify specific blood test alterations that were associated with poor outcome. Unfortunately, the studies were limited by size, different patient populations (e.g., geriatric population, surgical admissions), and differing study designs, including variable bloodwork and thresholds for individual tests. Decreases in Hgb and bicarbonate or increases in WBC or LDH were most frequently seen in patients with severe CI. More study is needed to clarify which serologic tests are most strongly associated with severe disease, which tests can best prognosticate outcome, and what threshold values are most sensitive and specific.
The differential diagnosis for patients presenting with abdominal pain and bloody diarrhea is broad, including Crohn’s disease, ulcerative colitis, infectious colitis, and colonic adenocarcinoma. Accuracy for the initial diagnosis of CI based upon clinical presentation is believed to be low. One retrospective study of all patients presenting to an emergency department in St Louis, Missouri, showed that of patients who presented with abdominal pain and bloody diarrhea and who were subsequently diagnosed with CI, only 9% were accurately identified at the time of presentation (109). Given the broad differential diagnosis and the inaccuracy of diagnosis based upon clinical presentation, initial evaluation for CI with serology and stool studies is very important. To properly assess the differential diagnosis, clinicians should consider initially obtaining complete blood count, comprehensive metabolic panel, stool culture, stool examination for ova and parasites, Clostridiumdifficile toxin assay, and serum lactate, LDH, creatine kinase, and amylase levels (Table 5). Complete blood count is useful to assess the WBC for prognostic purposes and the Hgb level to determine blood loss, although Hgb does not usually decrease significantly from baseline in patients with CI. Serum bicarbonate levels from electrolyte panels assess whether the patient is becoming acidotic, although serum lactate and LDH levels will also provide insight into the patient’s acid/base status. Stool culture and ova and parasite screens for infectious causes of bloody diarrhea are important initial studies. In one small study, Escherichia coli O157:H7 was identified by immunoperoxidase staining from colon biopsies in patients with pathologically supported CI (110); this organism may be etiologic for CI and should be tested for in all patients with bloody diarrhea. Although C. difficile infection infrequently presents with bloody diarrhea, given its increasing incidence and severity, it too should be part of the initial screening protocol for patients with bloody diarrhea. Elevations in serum amylase also have been shown to be associated with acute bowel ischemia (50). Despite none of these markers having sufficient evidence that they can diagnose CI, obtaining them during the initial workup may provide the clinician deeper insight into the likelihood and severity of CI.

Recommended initial serology and stool studies for suspected colon ischemia (CI)
IMAGING OF CI
Recommendations
- CT with intravenous and oral contrast should be ordered as the imaging modality of choice for patients with suspected CI, to assess the distribution and phase of colitis (strong recommendation, moderate level of evidence) (111, 112, 113).
- The diagnosis of CI can be suggested based on CT findings (e.g., bowel wall thickening, edema, and thumbprinting) (strong recommendation, moderate evidence) (111, 112, 113).
- Multiphasic CT angiography (CTA) should be performed on any patient with suspected IRCI or in any patient in whom the possibility of AMI cannot be excluded (strong recommendation, moderate level of evidence) (113, 114).
- CT or magnetic resonance imaging (MRI) findings of colonic pneumatosis and portomesenteric venous gas can be used to predict the presence of transmural colonic infarction (strong recommendation, moderate level of evidence) (115).
- In a patient in whom the presentation of CI may be a heralding sign of acute mesenteric ischemia (AMI; e.g., IRCI, severe pain without bleeding, and atrial fibrillation), and the multiphasic CT is negative for vascular occlusive disease, traditional splanchnic angiography should be considered for further assessment (conditional recommendation, low level of evidence) (114).
Summary of evidence
A variety of imaging methods have been used to diagnose CI, including plain films of the abdomen, barium enema (BE), CT, ultrasonography (US), and MRI. All can suggest or support the diagnosis, but none have findings that are specific enough to make a definitive diagnosis, except when infarction has occurred.
Plain films of the abdomen that show rounded densities along the sides of a gas-filled distended colon (“thumbprints”) and rigidity with thickening of the colon wall are suggestive of early ischemic change, whereas intramural gas (pneumatosis linearis), portal venous gas, and megacolon indicate advanced changes. In one retrospective report, suggestive signs of early disease were present in 21% of 41 patients with CI and no patient had the signs of more severe disease (116). When reversible CI was first described in 1963 by Boley et al. (117), serial BEs together with the patient’s subsequent course formed the basis for diagnosis. The original radiologic description of “reversible” CI was of “thumbprints” (pseudotumors) that were caused by subepithelial hemorrhage/edema and that either resolved in 1–2 weeks or evolved to a segmental ulcerative colitis picture with subsequent normalization over several months. Today, BE has a limited role in diagnosis and has been replaced by CT and colonoscopy (see below), largely because of the latter’s greater accuracy and ability to allow sampling of the mucosa for pathology. BE is now used primarily to follow the course of ischemic strictures, although virtual colonography or other imaging tests could be used for this purpose as well. In the usual scenario wherein the patient becomes asymptomatic after the index episode of CI, there are no data to support a benefit for repeating colonoscopy to prove the mucosa has returned to normal.
CT is commonly obtained in the emergency department to assess abdominal pain. When CT has not been obtained upon admission, the clinician should consider this modality when patients are classified as having either moderate or severe CI as defined in Table 6 (“Severity and Treatment of CI” section; see also Figure 1). These patients are at the highest risk for poor outcome and further characterization of the disease is helpful to determine appropriate management. CT is useful to exclude serious medical conditions other than CI (e.g., diverticulitis), can suggest the diagnosis of CI, and reveal which areas of the colon are involved. Segmental wall thickening, thumbprinting, and pericolonic fat stranding with or without ascites are signs associated with CI, but are not specific enough to make a definitive diagnosis. Wolff et al. (118) assessed patients with abdominal pain (with or without diarrhea or hematochezia) who had no history of gastrointestinal disease, who presented to the emergency department or were inpatients, and who had CT findings consistent with colitis and subsequent colonoscopy within 30 days of presentation; 36.4% of patients had ischemia as the etiology and no explanation of colitis was found in 26.1%. Fat stranding in the presence of bowel wall thickening was frequently seen in patients with diverticulitis, infectious colitis, and IBD, as well as in CI. This study confirmed that the usual CT findings of colitis are nonspecific and not unique for CI in most patients with abdominal pain (118).

Classification of disease severity and management

Diagnosis and treatment of colon ischemia (CI) based upon disease severity. BUN, blood urea nitrogen; CT, computed tomography; CTA, computed tomography angiography; Hgb, hemoglobin; IRCI, isolated right-colon ischemia; LDH, lactate dehydrogenase; MRI, magnetic resonance imaging; WBC, white blood cell count.
The appearance of thickened bowel wall in CI usually results from subepithelial edema and/or hemorrhage and reflects the evolving degree of ischemia and the time between the ischemic insult and performance of CT (111, 112). Balthazar et al. (111) published a retrospective case series of 54 patients with CI. The study subdivided the CT findings into three morphologically distinct groups based upon the timing of the examination in relation to the evolving pathophysiology. A “wet” appearance was seen in 61% of cases and appeared as a loss of colonic haustra with varying degrees of pericolic streakiness; this correlated to the acute pathologic changes after reperfusion of ischemic bowel. A “dry” appearance was seen in 33% of cases and manifested as concentric and symmetric mild mural thickening with homogenous attenuation of the colon wall and minimal pericolic streakiness; this correlated to the progression of ischemic damage without reperfusion. The remaining 6% had circumferential intramural air consistent with pneumatosis coli and presumed colonic necrosis (111). Of the overall cohort, 37% had moderate ascites and 24% had a “target sign” or “double halo” sign showing different attenuations of the layers of the bowel wall that corresponded to ischemia and reperfusion of the involved segment. This study attempted to characterize the most common findings in segments of colon affected by CI, but it lacked firm diagnostic criteria for CI, cohorts were relatively small, and there was no control group. Similar limitations are seen in the study of Romano et al. (112) that looked at patterns of CT signs in patients with early ischemia, late ischemia, and infarction. In this study, CI in 71 patients was classified based upon the phase of disease, and the authors described the “little rose” sign attributable to hyperdensity of the mucosa and edema of the submucosa as a sign of “early stage” CI, i.e., the “wet” appearance (112). Iacobellis et al. (119) retrospectively grouped CI in patients with pathologically proven disease and sequential CT imaging into acute (e.g., CT within 37 h of presentation), subacute (e.g., second CT between 37 h and 21 days), and chronic CI (e.g., third CT between 21 days and 2 months). When patients had no evidence of vascular occlusion, the acute phase was characterized by pericolic fluid (100%) and bowel wall thickening (28.1%); 86.4% had bowel wall thickening in the subacute phase. Bowel wall thickening was not frequently seen in patients with vascular obstruction in the acute or subacute phases (71.9%) and never in the chronic phase (119). None of these studies provided definitive criteria for diagnosis of CI using CT, although they offer some insights into potentially staging the ischemic process. Further investigation is required to characterize the most common signs of CI from each phase of the ischemic process and course of disease, to describe findings that reliably differentiate CI from other disease entities, and to determine what constellation of findings might be diagnostic of CI.
Adenocarcinoma of the colon is associated with CI and usually the segment of ischemic injury is proximal to the neoplasm. Tumoral segments can be differentiated from ischemic segments of colon by CT (120, 121). Ko et al. (122) looked at 20 patients who underwent CT, BE, and colonic resection because of adenocarcinoma of the colon with CI proximal to the tumor. On CT, the segments of CI had significantly less colon thickening (1.0 vs. 2.0 cm, P<0.05) and were longer (10.1 vs. 5.9 cm, P<0.05) than those with malignancy. In addition, although no statistical comparison was documented, the CI segments appeared to enhance more homogenously (70%), whereas the tumoral segments more frequently enhanced heterogeneously (60%) (122). This study is flawed by its small number of patients, lack of delineation of other CI findings, and absence of a true control arm, but it still offers some insight into the differences on CT between malignancy and segmental CI. Given the association, although infrequent, between CI and distal malignancy (as well as other potentially obstructing lesions such as strictures and fecalomas), the colon should be screened for cancer with a colonoscopy several weeks following recovery from the ischemic insult, if the patient has not been screened recently. Screening colonoscopy should not be performed at the time of presentation with CI because a minimum of colon manipulation and distension is recommended to avoid further damage from the reduction in blood flow that occurs with colon insufflation.
The etiology of CI is usually not identified, but in patients with known risk factors, CT might provide significant support for the diagnosis. Byun et al. (123) looked at 33 patients with lupus and acute abdominal pain: 79% of patients had evidence of ischemic bowel disease of whom 44% had ischemia involving the colon; the most frequent findings included engorgement of mesenteric vessels (79%), symmetric bowel wall thickening (74%), a target sign (67%), and multifocal bowel wall thickening (61.5%). Unfortunately, this study was small, did not compare its findings to a control arm, and lacked pathologic confirmation of the etiology of inflammation observed on imaging. Colonoscopy with biopsy remains the most accurate way to diagnose CI in patients with risk factors for disease, including vasculitides.
CI is usually nonocclusive in nature, but CT (or CTA) can be used to identify whether or not vascular occlusions are present. Unfortunately, the IMA is occluded in up to 10% of asymptomatic patients over 60 years of age and hence the significance of such a finding is uncertain (124). With emerging technology, contrast-enhanced CT can sometimes assess patency of the celiac, SMA, and IMA without devoted CTA; this usually requires direct communication with the radiology team to review the imaging specifically with the goal of vascular assessment. Data do not exist on the sensitivity and specificity of CT for assessing vascular occlusion in CI, but a meta-analysis including three prospective and three retrospective studies that looked at CT in the diagnosis of mesenteric arterial embolism, mesenteric arterial thrombosis, and mesenteric venous thrombosis (i.e., primary vascular AMI) found the sensitivity and specificity for diagnosis to be 93.3% and 95.9%, respectively (113). These six studies were performed in tertiary care referral centers in industrialized countries and, therefore, their high diagnostic accuracy might not reflect the accuracy of studies done in small community hospitals or practices; regardless, CT (or CTA) offers a high sensitivity and specificity for vascular assessment in patients with CI.
In contrast to AMI in which conventional mesenteric angiography or CTA plays an essential role, vascular imaging studies are not indicated in most patients with suspected CI because by the time of presentation, colon blood flow has usually returned to normal and the observed changes are not from ongoing ischemia but rather reflect the ischemic insult with or without reperfusion injury. In patients with potentially severe, complicated disease, such as those with IRCI or when the clinician cannot distinguish between AMI and CI (e.g., in patients with severe abdominal pain and little or no bleeding), a dedicated multiphasic CT is indicated. In patients with IRCI, CTA should be performed either initially or before discharge, as the colonic episode may be the “heralding” indication of SMA disease and possibly impending AMI. Multiphasic CT scanning, including a CT without oral contrast but with intravenous contrast and attention to the angiographic arterial and portal venous phases, has become standard for the diagnosis of AMI (125, 126, 127). One retrospective study that compared triple-phase CT scanning in 39 patients with pathologically confirmed AMI and 41 patients with suspected AMI who ultimately had another diagnosis showed that the specificity for detection of SMA thrombus or occlusion approached 100%, although the sensitivity was poor (26%). Similarly, for celiac and IMA thrombus, the specificity was estimated to be 98%, and the sensitivity was 5%. This study also showed that the diagnostic use of oral contrast during CT offered minimal additional benefit to the two vascular phases (114). Although this study contained small numbers of patients, it had a control group and characterized each phase of assessment, thus offering valuable data. In any patient in whom the presentation of CI may be a heralding sign of AMI (e.g., IRCI), and the multiphasic CT is negative for vascular occlusive disease, traditional splanchnic angiography should be considered for further assessment because a negative triple-phase CT does not absolutely exclude vascular obstruction as the cause. It is important to note that there are no available published data yet analyzing IRCI as a “heralding” indication of SMA disease. However, our experience has revealed that a select group of patients with IRCI may present again within weeks, months, or even a few years after the heralding presentation of IRCI with catastrophic episodes of AMI, resulting in loss of most of their small bowel or death. A limited but increasing number of patients with IRCI have undergone angiography and had occluding thrombi found in the SMA; stenting and/or thrombectomy resulted in good outcomes. Conversely, some patients with SMA thrombi did not undergo angiography or stenting yet had a positive outcome as well. Although there are no data to yet support our recommendation, we believe that the benefit of preventing a potentially catastrophic ischemic insult to the small intestine (AMI) far outweighs the risks of a CTA.
Pneumoperitoneum, portal venous gas, and pneumatosis are ominous findings in patients suspected of CI. In one Canadian study of 14 total patients who underwent colectomy with pathology showing transmural ischemia, CT showed that 100% had fat stranding, 71% had pneumatosis, and 36% had portal venous gas (128). However, the presence of pneumatosis and portal venous gas does not necessarily indicate nonviable bowel. In one small study of 23 patients with either small or large bowel ischemia, pneumatosis and portomesenteric venous gas were associated with transmural bowel infarction in 78% and 81% of patients respectively (129). When patients with an obstructing malignancy presented with a large bowel obstruction and CT showed cecal pneumatosis, surgery revealed transmural necrosis of the cecum in 26% of patients (6 of 23 total patients) (130). Milone et al. (115) assessed CT findings in 121 patients with transmural colon necrosis and 87 with limited colon necrosis. The presence of pneumatosis plus portomesenteric gas showed good specificity (83%) for transmural infarction, but very low sensitivity (17%); the concomitant presence of the two findings did not achieve statistical significance in predicting transmural CI (115). These studies are limited by their sample size and retrospective nature, but they do show that patients with CI who also have CT findings of pneumatosis and/or portomesenteric venous gas are likely to have severe disease, but not necessarily with full transmural necrosis. Nonetheless, in the clinical setting of CI, one of these findings is still an indication for prompt operation. Although CT has become the standard of care in assessing patients with suspected CI, both US and MRI also offer some diagnostic utility. In one retrospective case series of 58 patients with CI evaluated by US, the findings were as follows: symmetric bowel wall thickening (100%), segmental involvement of the colon (80%), preservation of colon wall stratification (66%), altered pericolic fat (28%), free fluid (19%), and pneumatosis (1.7%). When this cohort was subdivided into transmural necrosis and nontransmural necrosis, the only significant difference observed was the presence of abnormal pericolonic fat, which was seen more frequently in patients with transmural disease (75% vs. 20%, P<0.01) (131). In another study of 66 patients presenting to the emergency department with nonspecific abdominal pain who had abdominal US performed as their primary imaging modality, the group was subdivided based upon diagnosis into infectious colitis, inflammatory colitis, ischemic colitis, and malignant tumors. When the US findings were compared, arterial flow in the wall of the involved segments of colon was absent in 43% of those with CI compared with 12% of those with other diagnoses (P<0.05) (132). These US findings do not invalidate the reason why we do not recommend angiography in the evaluation of a first episode of CI, namely that by the time patients present with CI, colon blood flow has usually returned to normal, because they only measured signs of arterial flow in the bowel wall. This study was small and did not provide any criteria for the diagnosis of CI or information on the severity of the CI. Moreover, it is not known how many of the patients had infarcted bowel that, of course, would not have intramural flow. We would be hesitant to challenge this long-held belief until the results are confirmed in a robust manner. Experience with US in the setting of CI is very limited and it is believed that this technique lacks specificity for bowel wall thickening and has a high false negative rate (133).
MRI has been formally studied in only a small number of patients with CI; findings are similar to those of CT, but without the radiation exposure and the need for iodinated contrast agents. In one prospective study that assessed seven patients with CI, all of whom had an initial diagnostic CT and a subsequent MRI, similar segmental involvement and wall thickness were shown on both modalities (134). As with CT, such findings usually are not specific enough to make a definitive diagnosis. MRI may have a role when repeat imaging is required or patients have poor renal function.
COLONOSCOPY IN THE DIAGNOSIS OF CI
Recommendations
- Early colonoscopy (within 48 h of presentation) should be performed in suspected CI cases to confirm the diagnosis (strong recommendation, low level of evidence) (17).
- When performing colonoscopy on a patient with suspected CI, the colon should be insufflated minimally (conditional recommendation, very low level of evidence) (69, 135).
- In patients with severe CI, CT should be used to evaluate the distribution of disease. Limited colonoscopy is appropriate to confirm the nature of the CT abnormality. The endoscopic procedure should be stopped at the distal-most extent of the disease (strong recommendation, low level of evidence).
- Biopsies of the colonic mucosa should be obtained except in cases of gangrene (strong recommendation, very low level of evidence).
- Colonoscopy should not be performed in patients who have signs of acute peritonitis or evidence of irreversible ischemic damage (i.e., gangrene and pneumatosis) (strong recommendation, very low level of evidence).
Summary of evidence
Colonoscopy has become the primary technique to diagnose CI, usually after CT (see above) has revealed a segment of colon that is thickened with or without other more specific signs of ischemic damage, e.g., pneumatosis linearis and portal venous gas (see Figure 1). BE (see above) had been the main diagnostic mode in the 1960s but was gradually replaced by colonoscopy as the latter became increasingly available. Colonoscopy offers several advantages over radiologic imaging, including the ability to directly observe the abnormal tissue, to sometimes make a diagnosis just by appearance, and to obtain tissue samples. Nonspecific features of CI in addition to erythema, edema, and ulceration include aphthous ulcers, which may suggest Crohn’s disease, pseudomembranes, which are more often seen with C. difficile infection, and pseudopolyposis, which may develop with healing. Although the dusky, cyanotic hue of necrotic mucosa typifies gangrene and CI can be assumed in its presence, the validity of this assumption has never been tested. One retrospective study of 85 consecutive patients who had a colonoscopy to confirm diagnosis of CI showed that the most common findings in transient CI are edematous and fragile mucosa, segmental erythema, scattered erosions, longitudinal ulcerations, petechial hemorrhages interspersed with pale areas, purple hemorrhagic nodules, and a sharply defined segmental involvement (136). This study provides a clear description of the colonoscopic findings seen in patients with mild, transient CI, but it suffers from the flaws of many of the currently published studies that do not provide frequencies of these findings in the context of disease severity. Montoro et al. (17) looked at 297 patients who underwent colonoscopy for all levels of CI severity: findings were erythema (83.7%), edema (69.9%), friability (42.6%), superficial ulcerations including the single stripe sign (57.4%), deep ulcerations (21.7%), luminal narrowing and stenosis (8.4%), intraluminal blood (8.4%), and blue-black nodules with dark-dusky backgrounds suggestive of gangrene (5.5%). Scattered erosions may also be seen both proximal and distal to continuous segments of involvement.
The colon single-stripe sign (CSSS) is a highly specific sign of CI described by Zuckerman et al. (137) in 2003. CSSS is defined as a single inflammatory band of erythema with erosion and/or ulceration along the longitudinal axis of the colon; all CSSSs in the study of Zuckerman et al. (137) were >5 cm in length and 89% of CSSSs were found in the left colon. The 26 patients with CSSS had a better prognosis than did the 22 patients with circumferential CI and exhibited a reduced need for surgery (0% vs. 27%) and a lesser mortality (4% vs. 41%). Although of great interest, the study of Zuckerman et al. (137) was retrospective, small, had limited follow-up information, and a cause-and-effect relationship between ischemia and the CSSS was not proven.
Colonoscopy, in addition to detailing specific findings, also enables accurate determination of the anatomic limits of involvement and, therefore, perhaps helps predict prognosis. In 2010, Brandt et al. (7) showed CI that was isolated to the right side of the colon (IRCI) had a worse prognosis than CI involving any other anatomic segment of colon. In a multicenter Spanish study led by Montoro et al. (17) of 364 patients with CI, 345 of whom had colonoscopy, timing of colonoscopy was found to be important for diagnosis: when colonoscopy was performed within 48 h of presentation, typical hemorrhagic nodules were found in 47.1% of cases, but were evident in 33.3% of those in whom the examination was performed 2–5 days after presentation, and in only 9.7% of patients when colonoscopy was done after day 5. In 2011, in a retrospective study of 106 cases of CI divided into two groups, one with erythema and erosions and another with linear and circumferential ulcers, Beppu et al. (23) showed that CI was more severe with the latter pattern of disease; abdominal pain, C-reactive protein levels, and length of hospital stay were the only measures of severity given in this analysis that were significant. It is important to note that the correlation between endoscopic appearance and clinical severity is not absolute and even disease in patients with boggy, purple mucosa may resolve completely without complication. It is essential to assess the entire clinical picture before making any judgments about the need for surgical intervention. Finally, colonoscopy enables biopsy specimens to be obtained and, although uncommonly pathognomonic for CI, they often support the diagnosis, but rarely establish etiology. Risks of colonoscopy are small but must be considered in terms of the pathophysiology of CI. In 1969, Boley et al., showed that intraluminal pressures of the magnitude generated during colonoscopy and BE examinations, i.e., 30-60 mm Hg, reduced intestinal blood flow, especially to the mucosa, and caused shunting of blood from the mucosa to the serosa (48). In 1980, Kozarek et al. (135) showed that serosal splitting followed by mucosal tears, pneumatosis, and transmural perforation occurred in human cadaver colons at air pressures of 52–230 mm Hg, and intraluminal pressures that ruptured the cecum and sigmoid were 81 and 169 mm Hg respectively. They further showed during routine colonoscopy in three patients that intraluminal pressures ranged from 9 to 57 mm Hg when the tip of the colonoscope was free in the lumen of the bowel and 34–138 mm Hg when the tip was impacted against the colon wall (135). Carbon dioxide has been recommended for colonoscopy (and virtual colonography) because it is 10 times more rapidly absorbed from the bowel than is room air, and therefore its use results in a shorter period of distention and a more comfortable examination (138, 139, 140). In addition, Brandt et al. (69) showed that at all intracolonic pressures studied, CO2 increased colonic blood flow in contrast to room air that, at similar pressures, decreased blood flow, thus making CI less likely a complication of colonoscopy when CO2 rather than room air is used. However, CO2 has never been formally studied in humans with CI and all evidence presented is indirect. Despite this, CO2 appears to be the best insufflating agent to use in patients with CI and should be used whenever available.
There are currently no formal studies looking at perforation rates in patients undergoing colonoscopic evaluation of CI. The Brandt et al. (7) study cohort from 2010 included 251 patients who underwent a colonoscopic examination to the cecum using room air for insufflation; none of these colonoscopies were complicated by perforation (unpublished data). Of the 424 hospitalizations for CI observed by Longstreth and Yao (9), 408 colonoscopic evaluations were conducted using room air for insufflation, and again there were no documented perforations (unpublished data). In contrast to the assumed increased risks of endoscopic evaluation of CI, there does not seem to be a higher perforation rate in patients who undergo colonoscopic evaluation.
Limited colonoscopic evaluation is a safe and useful technique to evaluate patients with CI or suspected of having CI. CT should be used to characterize the stage of CI and the distribution of disease, but when colonoscopy is performed, the colonoscope should be passed only to the distal-most aspect of the affected region. Biopsies should be taken in all cases, except when there is evidence of gangrene.
Histopathologic specimens obtained colonoscopically are rarely diagnostic for CI. Pathognomonic features include infarction and ghost cells, i.e., preserved individual cellular outlines without cell content, and are infrequently seen (138). It is more common to see biopsy specimens showing mucosal and submucosal hemorrhage and edema and capillary fibrin thrombi with neutrophilic infiltration that are consistent with CI which, when taken in the context of clinical presentation, will support the diagnosis. Most commonly, pathologic features are nonspecific (138).
The diagnosis of CI, however, cannot be made conclusively by colonoscopy on just one examination unless mucosal gangrene is observed or infarction or ghost cells are seen at histopathology. Montoro et al. (17) found that of their 297 patients who underwent colonoscopy with biopsy, ghost cells and mucosal infarction were each seen in 7.7% of patients; of the 25 patients who had surgical resections, ghost cells and infarction were seen in 20% and 63%, respectively; thus, these histopathologic findings are infrequent and of limited value in diagnosing CI.
SEVERITY AND TREATMENT OF CI
Recommendations
- Most cases of CI resolve spontaneously and do not require specific therapy (strong recommendation, low quality of evidence) (107, 108, 139).
- Surgical intervention should be considered in the presence of CI accompanied by hypotension, tachycardia, and abdominal pain without rectal bleeding; for IRCI and pancolonic CI; and in the presence of gangrene (strong recommendation, moderate level of evidence) (17, 107, 108).
- Antimicrobial therapy should be considered for patients with moderate or severe disease (strong recommendation, very low level of evidence) (107, 108, 140).
Summary statement
- When considering the mortality risk for patients undergoing surgical intervention for acute CI, Ischemic Colitis Mortality Risk (ICMR) factors should be utilized (141, 142).
Summary of evidence
Surgical intervention and mortality are the most commonly used end points in studies that assess factors associated with poor outcome in CI and are used to define severe or complicated (poor outcome) disease in the data discussed below (Table 7). The strength of diagnosis from these studies is based upon the scheme presented in Table 8. Longstreth and Yao (9), Montoro et al. (17), and Brandt et al. (7) assessed large cohorts of patients looking at predictors of poor outcome, whereas Añón et al. (108), Huguier et al. (94), Lee et al. (24), O’Neill et al. (143), and Mosele et al. (107) each assessed smaller cohorts. These studies all conducted multivariate analyses and found various significant predictors of outcome including epidemiologic factors, clinical presentation of disease, vital signs, serologic values, and disease distribution. Epidemiologic factors that were associated with poor outcome included antimicrobial therapy for CI, hepatitis C positivity, history of cancer, male gender, and warfarin use at the time of diagnosis (9, 94, 107). The use of antimicrobial therapy is likely an indicator of the clinician’s response to disease severity rather than the antibiotic therapy per se contributing to poor outcome. Presentations of disease, e.g., abdominal pain without rectal bleeding, nonbloody diarrhea, peritoneal signs on physical examination and symptom onset after admission, are all associated with poor outcome (9, 17, 94, 107, 108, 143). A heart rate of >100 beats per min and systolic blood pressure of <90 mm Hg at the time of diagnosis are associated with the need for surgical intervention and/or mortality as are Hgb <12 mg/dl, hyponatremia (Na <136 mEq/l [mmol/l]), LDH >450 U/l, and blood urea nitrogen (>28 mg/dl [mmol/l]) (9, 17, 107, 108). As discussed previously, a pancolonic distribution of disease and IRCI also portend a poor outcome (7, 9, 107, 143). These studies were heterogeneous in terms of patient characteristics, physical examination findings, medical comorbidities, serology, and thresholds of various factors considered, but several risk factors appeared to be significantly associated with poor outcome in several of these studies: hypotension, tachycardia, abdominal pain without rectal bleeding, IRCI, and pancolonic CI.

Predictors of disease severity: factors from multiple studies that are significantly associated with the requirement for surgery and/or mortality

Modified Brandt and Boley 190 criteria for strength of diagnosis for colon ischemia (CI)a
Chung et al. (144) assessed 152 patients with clinically confirmed CI (74.5% confirmed pathologically) to analyze significant risk factors for poor outcome (e.g., improvement delayed by >2 weeks, 30-day colectomy, and 30-day mortality) and used these factors to devise a prognostic scoring system. The strongest predictors in decreasing order of significance were ulceration on colonoscopy, shock within 24 h of admission, and tachycardia at the time of diagnosis (144). If a patient had all three factors, their risk index for poor outcome was 74.5, whereas if ulceration and shock were present, but no tachycardia, the risk index decreased to 39.4; the risk index was 1.00 when none of these factors were present (144). This simple system is easy to use but requires further validation before being broadly applied, given their inclusion of patients with nonpathologically confirmed CI and including a nontraditional end point for severe disease (i.e., improvement delayed by >2 weeks). Ulceration seen on colonoscopy also has been associated with poor outcome in a study by Matsumoto et al. (139). This small study using clinical diagnostic criteria showed that patients with ulceration on colonoscopy required longer periods of fasting and had a longer duration of admission before clinical improvement compared with those without ulceration. This study was very small but is a reinforcement of the importance of mucosal ulceration as a predictor of outcome in patients with CI.
In view of the above data and previously described diagnostic options, this guideline proposes redefining disease severity to guide treatment (Table 6 and Figure 1). This is currently a nonvalidated guide to rating disease severity but incorporates the most up-to-date knowledge of risk factors for disease severity. Patients with mild disease are those who have typical symptoms of CI with a segmental colitis not isolated to the right colon and with none of the commonly associated risk factors for poorer outcome that are seen in moderate disease. Moderate disease includes any patient with up to three of the following factors: male gender, hypotension (systolic blood pressure <90 mm Hg), tachycardia (heart rate >100 beats/min), abdominal pain without rectal bleeding, blood urea nitrogen >20 mg/dl, Hgb <12 g/dl, LDH >350 U/l, serum sodium <136 mEq/l (mmol/l), WBC >15 × 109/l, or colonoscopically identified mucosal ulceration. Severe disease is defined by more than three of the previously listed criteria or any of the following: peritoneal signs on physical examination, pneumatosis on CT, gangrene on colonoscopy, and a pancolonic distribution or IRCI on CT or colonoscopy.
Treatment of CI varies with the severity of the disease and its presentation. In general, many patients have a benign, self-limited episode of CI that is neither diagnosed nor treated or is managed in the outpatient setting. Most cases of CI resolve spontaneously and do not require specific therapy; such patients have reversible ischemic colopathy or transient ischemic colitis (91). Patients with more significant symptoms or findings require hospitalization to enable observation for complications or signs of irreversible disease. Initial medical management most commonly includes general supportive measures, bowel rest, intravenous hydration, and correction of possible precipitating conditions. Parenteral nutrition may be indicated if a protracted course is anticipated. No therapeutic modality has ever been tested in a rigorous clinical trial and the mostly benign nature of CI has led to a shortage of trials assessing various therapies. It is also important to consider that the currently available literature for the management of CI focuses on hospitalized patients who have complicated disease with less emphasis on the milder cases that are not hospitalized. The recommendations presented in this guideline are mostly based on small retrospective studies that lack control groups. Most guideline statements are based upon extrapolation from the available literature and expert opinion.
One systematic review of the management of CI included 10 retrospective studies comprising 841 patients (145). Within these studies there was no standard protocol for management; however, nonsurgical treatment usually included bowel rest, intravenous fluid, electrolyte repletion, and antibiotic usage with occasional administration of total parenteral nutrition. All articles reviewed did agree that surgery was indicated for patients with peritonitis or those who were hemodynamically unstable (145). This systematic review had significant limitations including methodologic anomalies such as excluding some well-structured publications and also including three studies with patients who had CI as a complication of vascular procedures despite methodology stating this as a criterion for exclusion. In addition, the study included some patients without pathologically confirmed disease. This lack of uniformity characterizes the CI management literature, but the abstract’s conclusion reads “There is very little evidence base for the management of this condition” (145). We believe this statement is accurate.
O’Neill et al. (148) conducted a subsequent systematic review of the management of CI, attempting to improve on the methodologies from Diaz-Nieto et al. (145). This review provided a more rigorous screening evaluation of the studies by including only biopsy-proven disease in each patient and excluding all studies with CI resulting from vascular surgery or associated with colonic adenocarcinoma (148). Eight retrospective case-series and three case-control studies comprising 1049 patients were included. Overall, 80.3% of cases were medically managed without surgical intervention and had a 6.2% mortality rate; 19.6% were managed surgically with a mortality rate of 39.3% (148). These data offer the best overall insight into medical vs. surgical management of CI and associated outcomes. This analysis is also consistent with the presumption that those requiring surgery are the sickest and at highest risk for poor outcome. Medical management most commonly included fasting, intravenous fluids, parenteral nutrition, antibiotics, and heparin prophylaxis (148). Requirement for pathologic confirmation of disease is a strength of this study, and is also a marker of disease because colonoscopy or surgical intervention isolates those with more advanced disease or when the diagnosis might be unclear. There was, however, also significant heterogeneity among the algorithms used in various studies for medical management of disease, with some including and others excluding, antimicrobial therapy, and none detailing the frequency, duration, or type of antibiotics used.
Indication and timing for antimicrobial use in CI remains untested. There is no clinical evidence to show beneficial effects of such therapy and it is unlikely that a randomized controlled trial will be forthcoming; because the prognosis of CI is excellent in most cases, the number of patients in such a trial needed to show benefit (or to disprove a lack of benefit) would have to be immense. Previous recommendations for antibiotic usage were based on experimental studies that showed reduction in the severity and extent of bowel damage when antibiotics were given before or during an ischemic event, with the majority of these trials being several decades old (140, 146, 147, 149, 150). Yoshiya et al. (140) pretreated mice with ampicillin, vancomycin, neomycin, and metronidazole, and subsequently induced intestinal ischemia with reperfusion by ligating the SMA for 30 min. These mice were then compared with control mice that also underwent intestinal ischemia but did not receive antimicrobial therapy. In the mice pretreated with antibiotic therapy, the expression of Toll-like receptors 2 and 4 was decreased as was expression of inflammatory markers (e.g., tumor necrosis factor, interleukin-6, and cyclo-oxygenase-2). As Toll-like receptors normally bind Gram-positive and Gram-negative bacteria to stimulate inflammatory responses, the study supports the theory that antimicrobial therapy decreases the overall inflammatory response to ischemic injury. Intestinal injury resulting from ischemia and reperfusion is also believed to be stimulated by ischemic cells presenting neoantigens that bind natural immunoglobulins to activate the complement pathway. Yoshiya et al. (140) also showed decreased complement (C3), IgM, and IgA in ischemic tissue of mice pretreated with antimicrobials compared with the ischemic tissues of mice not exposed to antimicrobial therapy.
Antimicrobial therapy is also believed to prevent poor outcome through decreased bacterial translocation in the setting of acute ischemia and reperfusion injury. The loss of mucosal integrity as a result of vigorous inflammation has been shown in mouse models to facilitate bacterial translocation and resulting bacteremia (151, 152, 153). Luo et al. (153) studied mice that had ischemia induced by SMA occlusion for 30, 60, or 90 min followed by reperfusion for 30 min. These mice were given varying oral doses of bacteria after the ischemic episode and had blood cultures drawn immediately and 15 min after reperfusion. A control group of mice was fed the same bacteria but did not have any ischemic episode. Control mice showed no translocation of bacteria, whereas the mice that were exposed to even 30 min of ischemia and a low bacterial inoculum developed bacteremia (153). The studies of Yoshiya et al. (140) and Luo et al. (153) reinforce the theories behind antimicrobial therapy in the setting of CI in mouse models. Antibiotics are believed to improve outcome in CI by reducing inflammatory responses stimulated by the normal fecal microbiome, reducing the antigens that prompt innate immune response and minimizing bacterial translocation through compromised colonic mucosa.
Available human studies of antimicrobial treatment in CI are few in number, heterogeneous in design, and do not directly address antimicrobial use for a specific therapeutic benefit. Three studies have presented data regarding broad-spectrum antimicrobial therapy of CI and associated outcomes (107, 108, 139). Añón et al. (108) looked at 85 consecutive patients, of whom 69 had “mild disease” that was treated with fluid and electrolyte correction and “wide-spectrum antibiotics”; all but 1 patient survived (98.6%) and another 16 patients had severe disease that was initially treated medically, but subsequently required surgery. Mosele et al. (107) retrospectively assessed 46 patients who were at least 65 years of age, of whom 67.4% clinically improved with only medical therapy consisting of intestinal rest, total parenteral nutrition, and broad-spectrum antibiotics; 6 of the original cohort received medical therapy and subsequently died (13.0%), whereas another 9 would ultimately require surgical intervention (19.6%). Matsumoto et al. (139) retrospectively assessed 41 patients with CI, with 31.7% of patients receiving a “combination of antibiotics” along with fasting, bowel rest, and fluid replacement; none of these patients required surgery or died. These studies are similar as they were all small, not designed to assess the effect of antimicrobial therapy on outcome, mentioned antimicrobial therapy as part of the medical treatment regimen but mostly did not detail the number of patients within the “medical therapy” cohort who received antibiotics, and did not delineate the specific antibiotics used or the duration of therapy. Perhaps most importantly, there were no comparator groups of patients who did not receive antimicrobials.
By performing multivariate analysis on 401 consecutive patients, Longstreth and Yao (9) found that antimicrobial therapy was associated with a 3.94 (confidence interval: 1.23–164, P<0.05)-fold increased risk of severe disease as defined by need for surgery or mortality. This finding speaks to one of the major weaknesses of all available treatment data, namely that this statistical association is likely the result of a selection bias by which patients with the most severe disease are those receiving antimicrobial therapy, most of whom are most at risk for poor outcomes regardless of therapy.
Because there is a shortage of clinical trials of antimicrobial therapy in CI and there is experimental evidence that these medications should be beneficial, this guideline recommends antimicrobial therapy for CI patients who have either “moderate” or “severe” disease as newly classified in a previous section of this guideline (see also Figure 1). The criteria for classification are based upon risk factors for poor outcome in CI that is believed to be mediated through a vigorous inflammatory response, bacterial translocation, and extensive damage to the large bowel. Mouse models have shown antimicrobial use moderates these processes and we believe these will improve outcome in the appropriate clinical setting. This recommendation is based upon expert opinion considering the murine models, retrospective human studies, and personal experience. As previously discussed, it is highly unlikely that a properly designed randomized control trial of antibiotics in humans stratified for mild, moderate, and severe CI will ever be performed.
The question of which antimicrobial agents are most efficacious in patients with CI is also unanswered. Plonka et al. (154) transected the vascular supply to the colon in mice and then treated them with saline, gentamicin alone, metronidazole alone, or gentamicin plus metronidazole. Mice receiving metronidazole alone or gentamicin plus metronidazole showed improved survival. This study supports the role of anaerobic bacteria as a contributing factor to poor outcome. Because of the risks of bacterial translocation across compromised colonic mucosa, with inflammatory and innate immunologic reactions that are stimulated by the colonic microbiota, we recommend a broad antimicrobial regimen to “cover” these organisms. Possible antimicrobial regimens include an anti-anaerobic agent plus a fluoroquinolone or an aminoglycoside or a third-generation cephalosporin.
The optimal duration of antimicrobial therapy is unclear and studies to date have not addressed this issue. Once therapy has been initiated, this guideline recommends that antimicrobials be continued for at least 72 h, at which time the patient’s clinical status should be reevaluated. If the patient has not clinically improved, one should consider consultation with an infectious disease expert to help define the antimicrobial regimen. If the patient is symptomatically improved after 72 h, a 7-day course of therapy should be considered.
Glucocorticoids are not recommended for CI, except when it is a complication of a vasculitis. In such cases, the steroids are used to treat the vasculitis and not the CI. The only potential role for these agents or others used in the treatment of IBD might be in patients with chronic CI (see above), but there is no published experience to support the use of local or systemic glucocorticoids, sulfasalazine, aminosalicylates, or fatty acid enemas to treat CI. Indeed, there are numerous reports implicating these drugs as a cause of CI and, in one experimental study using Fischer rats, azathioprine and methylprednisolone augmented the damage of intestinal ischemia (155). Nonsteroidal anti-inflammatory drugs are generally accepted to be a cause of colonic ulcerations, but one large trial of patients with CI showed that a lack of nonsteroidal anti-inflammatory drug use at the time of diagnosis was independently associated with severe disease (e.g., surgery and/or death) (9). This potentially protective effect of nonsteroidal anti-inflammatory drugs was an indirect observation with no further trials to date (9). Anecdotal evidence has shown that fatty acid enemas have helped to heal the necrotic mucosa of two patients with otherwise unresponsive CI, although there are no formalized publications supporting this intervention (LJ Brandt and SJ Boley, unpublished).
Surgical intervention for patients with CI is required in its most severe presentations. The O’Neill et al. (148) review of 11 studies comprising 1,049 patients showed that 19.6% of pooled patients required surgical intervention and had a mortality rate of 39.3%. Published data have wide ranges for the need for surgery and vary with the study population (e.g., surgical service vs. general population; age >65 vs. <65 years); 8–19.8% of large, broad populations with biopsy-proven CI have been estimated to require surgical intervention, whereas the need for surgery in patients admitted to surgical services is as high as 45.2% (7, 9, 94). The requirement of biopsy-proven disease in some studies mandates endoscopic evaluation, thereby perhaps excluding patients not sick enough to warrant colonoscopy, biasing the study population to patients who are more acutely ill, and overestimating the true need for surgical intervention. Inclusion of patients on a surgical service is not representational of a general population and cannot be applied to all patients with CI. Given the mostly benign course of CI, and the fact that many patients with CI do not present to medical attention, estimates of the frequency of surgery in hospitalized patients with CI is likely a significant overestimation. We recommend considering surgical consultation if patients fulfill the risk stratification for moderate or severe disease as these factors are associated with need for surgery and/or mortality.
There are several indications for surgery in acute CI, but the most common is the presence of signs of necrotic bowel (Table 9). These might include peritoneal signs on physical examination, pneumatosis or portal venous gas on radiologic imaging, or gangrene on colonoscopic examination. Without surgical intervention, mortality from necrotic bowel approaches 100%. Following the new classification scheme proposed here, patients with “severe disease” would require emergent surgical consultation. The current literature does not clarify surgical indications or optimal timing for surgical intervention. Huguier et al. (94) assessed 33 patients who underwent surgery for CI, 13 of whom had immediate surgery (i.e., <12 h after admission) for “abdominal tenderness,” with 5 having peritonitis upon surgical inspection and 8 expiring; 20 patients had delayed surgical treatment (i.e., days 2–7 of hospitalization) for clinical deterioration after admission, with 6 subsequently dying from complications of CI. Patients who develop a segmental colitis pattern during the evolution of their disease and whose symptoms persist for more than 2–3 weeks or who have a continuing protein-losing colopathy for several weeks usually are best treated by segmental colectomy. A less-recognized indication for surgery is the development of recurrent sepsis in a patient who has symptomatically recovered from an acute episode of CI. Such patients usually have a short segment of unhealed bowel that, via bacterial translocation, is the source of the sepsis; resection of this segment is curative.

Indications for surgery in colonic ischemia
The surgical procedure patients undergo for CI depends upon the affected segment of colon, but most commonly include total or subtotal colectomy, right hemicolectomy, or segmental colectomy with either a primary anastomosis or diverting stoma (Table 10). Antolovic et al. (156) prospectively collected data on patients requiring surgical intervention at the University of Heidelberg between 2001 and 2004. Of the 85 consecutive patients undergoing surgery, 56 (66.7%) required procedures within 24 h of presentation to the surgical service. Left hemicolectomy was performed in 8%, right hemicolectomy in 26%, sigmoid resection in 5%, and total colectomy in 49%, with the remainder having other segmental resections; 42% had a Hartmann procedure and another 38% had a diverting stoma created in addition to bowel resection (156). Castleberry et al. (141) retrospectively assessed 115 consecutive patients undergoing surgery for acute CI: segmental colon resection was most common (53%), with right hemicolectomy (49%) being the predominant segmental resection performed; 26% had subtotal or total colectomy, 10% had ileocecectomy, and 10% had a Hartmann procedure; 87% of patients also required an ileostomy or colostomy. Reissfelder et al. (142) prospectively assessed 177 consecutive patients undergoing surgical management for acute CI between 2002 and 2008. Subtotal colectomy was performed in 54%, right hemicolectomy in 38%, and left hemicolectomy in 8%; 61% of their patients had a stoma placed (142). These studies provide a cross-sectional view of surgical treatment patterns for CI, but of course do not assess which surgical procedure is most efficacious for which presentation. The choice of surgical procedure is influenced by a number of factors including the training of the surgeon and his or her practice patterns.

Surgical resection and in-hospital mortality
Mortality after surgical intervention for CI is high, ranging from 37 to 47% (141, 142, 156). Risk factors for postoperative mortality are more definable than most factors associated with CI, given the fact that the diagnosis is known after surgery, the disease is acute, and the various clinical factors can be quantified. Antolovic et al. (156) assessed 85 consecutive patients with acute CI undergoing surgery and found a mortality rate of 47%. American Society of Anesthesiologists Status (ASA) >3, emergency surgery, and blood loss >300 ml were each independent and strong predictors for mortality. Reissfelder et al. (142) conducted a retrospective analysis of 177 consecutive patients and identified low-output heart failure (e.g., cardiac ejection fraction <20% on echocardiogram), acute kidney injury, lactate >2.5 mmol/l, subtotal colectomy, and pre- and intraoperative catecholamine administration as being the risk factors associated with high perioperative mortality rate. This study then showed that if one point was given for each of the listed risk factors, mortality increased from 10.5 to 100% as points increased from 0 to 5 respectively (Table 11). This classification scheme was termed the Ischemic Colitis Mortality Risk Score (ICMR) (142). Castleberry et al. (141) retrospectively assessed 115 patients who underwent surgical treatment of their CI to assess for factors associated with postoperative mortality and to validate the ICMR. 37% of the patients died in the postsurgical hospitalization period and multivariate predictors of mortality were as follows: ASA class >4 (odds ratio (OR): 6.91, confidence interval (CI): 2.17–30.98, P<0.001), peak preoperative lactate level (OR: 1.26, CI: 1.11–1.47, P<0.001), postoperative dialysis requirement (OR: 5.11, CI: 1.72–16.88, P<0.001), intraoperative adrenergic vasopressor requirement (OR: 2.07, CI: 1.47–8.82, P<0.01), total ICMR score (OR: 2.11, CI: 1.44–3.22, P<0.001), and blood loss >500 ml (OR: 2.63, CI: 1.00–7.21, P<0.05) (141). Despite the ICMR score being predictive of mortality when its individual components were considered, only elevated preoperative serum lactate (P<0.01), renal failure requiring hemodialysis (P<0.01), and intraoperative vasopressor requirement (P<0.01) were significantly associated with poor outcome, whereas low cardiac output and whether subtotal or total colectomy was performed were not associated (141); risk stratification using ICMR was validated in this study. There are some limitations of the ICMR including the challenges with differentiating occlusive from nonocclusive CI in the acute setting and that mortality associated with colectomy might result from other factors and not the surgery per se (e.g., the extent of colonic injury, significant blood loss, or overall hemodynamic instability). This guideline recommends that ICMR should be considered as part of the risk assessment of patients with acute CI who need surgical intervention.

Risk factors for perioperative mortality
Colon stricture after an episode of CI may be asymptomatic or even resolve over months to years. Surgery is indicated only when an ischemic stricture produces symptoms; in such cases, segmental resection is adequate. Transendoscopic dilation of an ischemic stricture is an alternative to surgery, although an unproven one. Chronic segmental CI is a more controversial indication for surgery and, as with other colitides, the decision to abandon medical therapy is a complex one that must be individualized for each case. Recurrent CI is uncommon and resection of the involved segment of colon, while usually curative, does not necessarily protect against recurrent CI in other areas of the colon. There are no published data on the frequency of such recurrence following surgery for recurrence.
Treatment of CI depends upon disease severity at presentation (see Figure 1). The overwhelming majority of patients will require simple conservative measures to manage their disease including fasting, intravenous fluids, and correction of underlying conditions. If patients have moderate or severe disease, broad-spectrum antimicrobial coverage should be instituted along with surgical evaluation. Surgery should be consulted promptly for patients with severe disease or colon necrosis.
ACKNOWLEDGMENTS
This guideline was produced in collaboration with the Practice Parameters Committee of the American College of Gastroenterology. The Committee gives special thanks to Fouad J. Moawad, MD, FACG, who served as guideline monitor for this document.
REFERENCES