ACG Clinical Guideline: Diagnosis, Treatment, and Prevention… : Official journal of the American College of Gastroenterology
Introduction
Acute diarrheal infection is a leading cause of outpatient visits, hospitalizations, and lost quality of life occurring in both domestic settings and among those traveling abroad. The Centers for Disease Control and Prevention has estimated 47.8 million cases occurring annually in the United States, at an estimated cost upwards of US$150 million to the health-care economy (1, 2). Acute diarrhea can be defined as the passage of a greater number of stools of decreased form from the normal lasting <14 days. Some definitions require an individual to present with an abrupt onset 3 or more loose or liquid stools above baseline in a 24-h period to meet the criteria of acute diarrhea. Persistent diarrhea is typically defined as diarrhea lasting between 14 and 30 days, with chronic diarrhea generally considered as diarrheal symptoms lasting for greater than a month. Acute diarrhea of infectious etiology is generally associated with other clinical features suggesting enteric involvement including nausea, vomiting, abdominal pain and cramps, bloating, flatulence, fever, passage of bloody stools, tenesmus, and fecal urgency. Acute diarrheal infection is also often referred to as gastroenteritis, and some acute gastrointestinal infections may cause a vomiting predominant illness with little or no diarrhea.
This guideline provides recommendations for the diagnosis, management, and prevention of acute gastrointestinal infection focusing primarily on immune-competent adult individuals and does not consider Clostridium difficile-associated infections, which has recently been reviewed in a separate American College of Gastroenterology (ACG) Clinical Guideline (3). It replaces a previously published ACG Guideline on the same topic (4), and supplements previously published Infectious Disease Society of America (IDSA) (5), and World Gastroenterology Organization guidelines (6). This guideline is structured into five sections of clinical focus to include epidemiology and population health, diagnosis, treatment of acute disease, evaluation of persisting symptoms, and prevention. To support the guideline development, a comprehensive literature search on acute diarrheal infection in adults was performed across multiple databases. A medical library information specialist searched the Ovid MEDLINE and EMBASE databases for relevant articles on 18 February 2015, using the following main terms (with synonyms and closely related words): “diarrhea” AND “acute disease,” “infectious diarrhea”, “dysentery,” or “acute gastroenteritis.” The searches were limited to English language articles published in the past 10 years and excluded case reports, and child or animal studies. Details of the search methodologies are provided in the Appendix. Additional articles were obtained from review of references from retrieved articles, as well as articles that were known to authors.
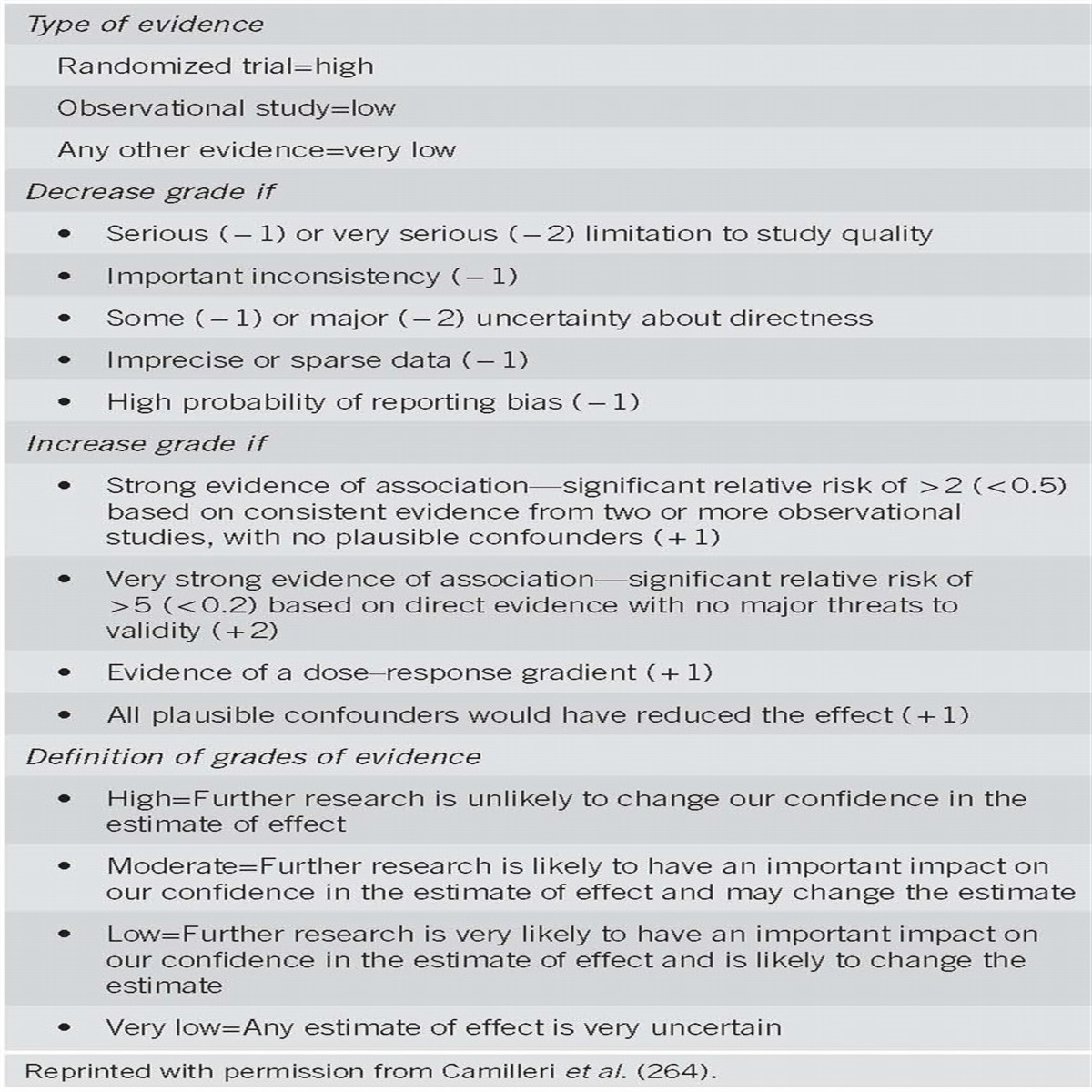
Each section presents key recommendations followed by a summary of the evidence (Figure 1 and Table 1). The GRADE system was used to grade the strength of our recommendations and the quality of the evidence (7). The strength of a recommendation is graded as “strong,” when the evidence shows the benefit of the intervention or treatment clearly outweighs any risk, and as “conditional,” when uncertainty exists about the risk–benefit ratio. The quality of the evidence is graded as follows: “high,” if further research is unlikely to change our confidence in the estimate of the effect; “moderate,” if further research is likely to have an important impact and may change the estimate; “low,” if further research is very likely to change the estimate; “very low,” if an effect is very uncertain (8).

Summary and strength of recommendations

Approach to empiric therapy and diagnostic-directed management of the adult patient with acute diarrhea (suspect infectious etiology).
Epidemiology and public health considerations
Recommendation
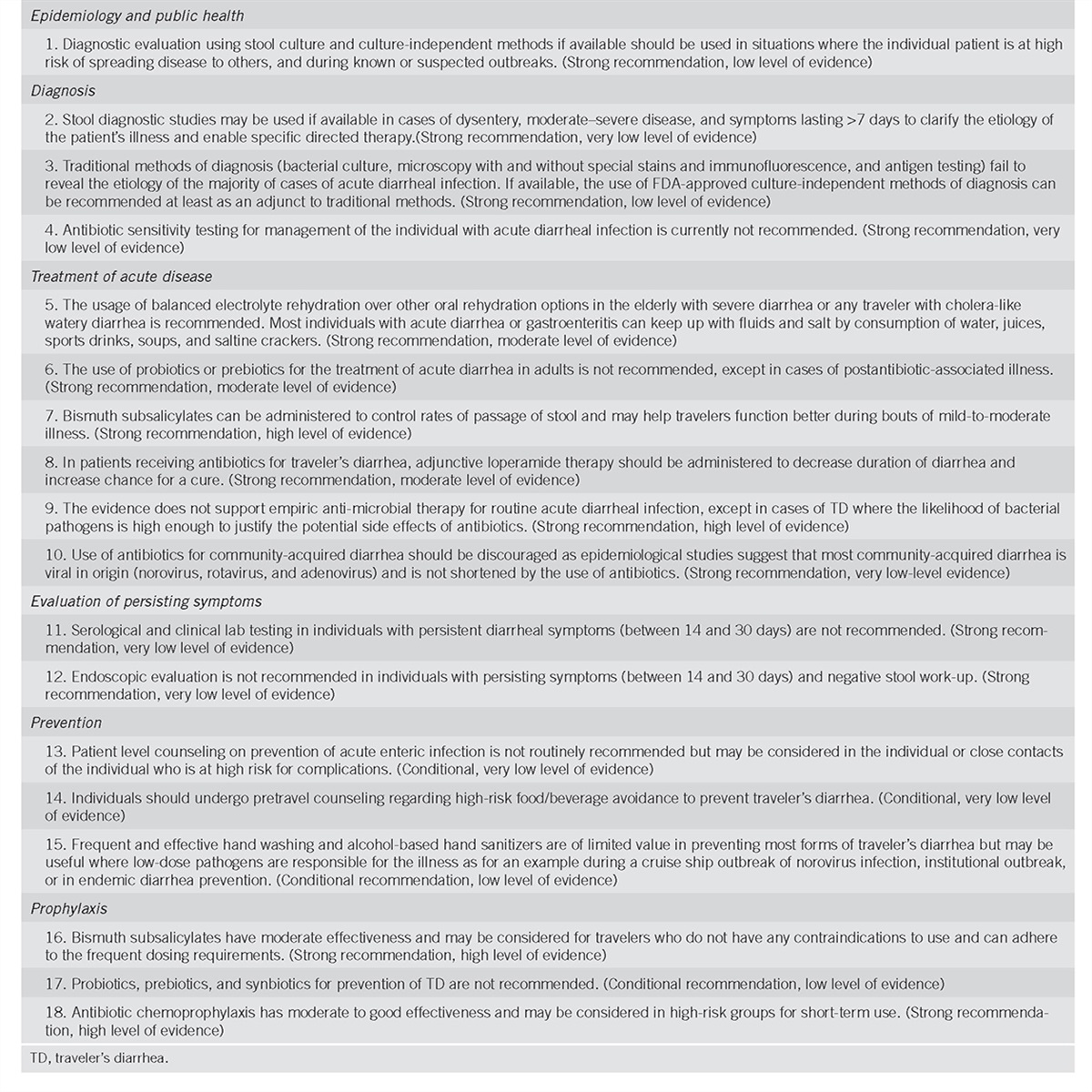
1. Diagnostic evaluation using stool culture and culture-independent methods if available should be used in situations where the individual patient is at high risk of spreading disease to others, and during known or suspected outbreaks. (Strong recommendation, low level of evidence)
Summary of evidence
Surprisingly, there are few published studies that describe the overall incidence of acute diarrhea (including infectious and non-infectious causes) in the United States. In 1998, the Foodborne Diseases Active Surveillance Network (FoodNet) conducted a random population-based telephone survey in which 12,755 persons (median age 40 years) were interviewed (9). Overall, 6% reported having experienced an acute diarrheal illness at some point during the 4 weeks preceding the interview (overall annualized rate, 0.72 episodes per person-year; 15–24, 1.1 episodes per person-year; 25–44, 1.7 episodes per person-year; 45–64, 1.2 episodes per person-year). A follow-up survey where 3,568 respondents (median age 51) were asked at random about illness in the previous 7 days or previous month found that recall bias had an important effect on estimates of acute gastrointestinal illness (10). Using a 7-day exposure window, the estimated incidence of acute diarrhea was 1.6 episodes per person-year, compared with 0.9 episodes per person-year if asked about illness within the preceding month. Other population-based studies from Canada and western European countries using varied methodologies estimate annual incidence between 0.1 to 3.5 episodes per person-year (11).
Specifically focusing on infectious causes of acute diarrheal illness, in 2011 the Centers for Disease Control and Prevention updated the estimates of infectious gastroenteritis caused by a myriad of viruses, bacteria, and parasites (1, 2). Based on empirical modeling of active, passive, and outbreak surveillance data ˜47.8 million foodborne-related illnesses occur annually (one out of every six persons) in the United States. Furthermore, it was estimated each year that 31 major pathogens acquired in the United States caused 9.4 million episodes of diarrheal illness, 55,961 hospitalizations, and 1,351 deaths. In addition, unspecified agents resulted in 71,878 hospitalizations and 1,686 deaths, caused ˜38.4 million episodes of domestically acquired foodborne illnesses. In addition to domestically acquired infections, over 44 million US residents traveled abroad to non-Canadian and non-European destinations in 2014 (12), resulting in roughly 4 to 17 million cases of traveler’s diarrhea (TD) based on 10–40% attack rates (13). In addition to the significant burden of the acute illness associated with these infections, recent evidence suggests that these pathogens are linked with chronic health sequelae, including functional gastrointestinal disorders, reactive arthritis, hemolytic uremic syndrome, and Guilliane Barré syndrome (14, 15, 16, 17, 18, 19, 20). The cost of acute and chronic illness attributable to these infections is estimated to be upwards of US$145 billion to the US economy (21, 22, 23).
In light of these data, acute diarrheal illness is considered a major public health issue against which control efforts are needed. While this guideline is primarily focused on the diagnosis, prevention, and treatment of acute diarrhea in the individual, it is appropriate to specifically address the importance of diagnosis of the individual in the context of population health improvement. Public health surveillance and response in the field of acute diarrhea include strategies of infection control, anti-microbial stewardship, outbreak investigation, as well as food and water safety interventions and regulatory policy (24). The individual patient–medical encounter is the interface and provides critical input on which the success of these control strategies are built. There are significant data gaps and limitations with current burden of disease estimates that are due to limitations in the current reporting structure (2, 25). Important multipliers for which there is significant uncertainty in published burden of disease models include the underreporting multiplier (which adjusts data reported to health departments as part of routine public health surveillance for the number of infected people who seek treatment and test positive for a specific infectious agent), and the pathogen fraction multiplier (which is used to attribute a proportion of all episodes of gastroenteritis to particular pathogens) (25). Improvement of estimates, which is required to make important policy decisions, benefits from more certain data that comes from better reporting. From an outbreak investigation perspective, culture-based testing and reporting (and advanced isolate characterization) is needed to provide sufficient information to distinguish among strains or serotypes and perhaps identify virulence characteristics and susceptibility to anti-microbial agents that relies on testing individual cases (26). Established networks such as FoodNet and Pulsenet have demonstrated the importance of active surveillance for examining trends in specific diseases over time, evaluating impact of food safety policy, as well as identifying and responding to large common source outbreaks (27).
However, a comprehensive laboratory evaluation and advanced characterization work-up is neither practicable nor cost-effective for every patient presenting with an acute diarrheal infection (28). No formal cost-effectiveness studies on the optimization of testing and reporting has been reported and these would be challenging to conduct. However, public health fundamentals would strongly support individual patient testing and reporting in a number of situations. These include diarrhea outbreaks among workers who prepare and handle food, health-care workers, daycare (adult and child) attendees/employees, and residents of institutional facilities (3). Additionally, if testing is conducted for individual clinical reasons, the results of these tests should be reported to public health authorities in compliance with both voluntary and mandatory state requirements on reportable events.
Finally, with the advent of growing availability and increasing use of culture-independent technologies in clinical laboratories (discussed in detail later), an emerging concern is the potential impact on replacement of culture-based methods for the aforementioned public health utilization (26). Current public health and control strategies rely on isolate recovery, specimen preservation, and partnerships with clinical laboratories. Although culture-independent methods provide a promise for more sensitivity of pathogen identification (leading to more accurate disease-burden estimates), they do so with a detrimental impact on the advanced characterization and typing, which is needed in outbreak investigation and resistance monitoring efforts. As such, and until new methods have evolved in which genotypic advanced characterization platforms are widely available, it is recommended that culture-based and culture-independent testing be used in parallel when practicable to support public health purposes.
Diagnosis
Recommendations
2. Stool diagnostic studies may be used if available in cases of dysentery, moderate-to-severe disease, and symptoms lasting >7 days to clarify the etiology of the patient’s illness and enable specific directed therapy. (Strong recommendation, very low level of evidence)
3. Traditional methods of diagnosis (bacterial culture, microscopy with and without special stains and immunofluorescence, and antigen testing) fail to reveal the etiology of the majority of cases of acute diarrheal infection. If available, the use of Food and Drug Administration-approved culture-independent methods of diagnosis can be recommended at least as an adjunct to traditional methods. (Strong recommendation, low level of evidence)
4. Antibiotic sensitivity testing for management of the individual with acute diarrheal infection is currently not recommended. (Strong recommendation, very low level of evidence)
Summary of the evidence
The commonly accepted statement that specific investigation is not normally required in the majority of cases of acute watery diarrhea because it is usually self-limiting and resolves without specific treatment may under inform the ability to provide a more rapid resolution of symptoms with appropriate directed therapy and potentially prevent postinfectious sequelae (29). Historical guidelines for diagnostic testing (ACG, IDSA) seem to be too restrictive in the current environment of new diagnostic methods and enhanced ability to target therapy (4, 5).
Evidence supporting the use of diagnostic testing to support clinical management may be different in higher-resource settings than they would be, for example, in the traveler who is in an area with limited access to adequate medical care or diagnostics (30). Appropriate microbial identification may be helpful in tailoring therapy as in antibiotics for bacterial pathogens, supportive therapies, and avoidance of antibiotics for viral pathogens or more specific anti-microbials for parasitic protozoan etiologies. As symptoms of acute diarrhea are protean, attempts to diagnose etiologic agents or classes are subjective at best and fraught with imprecision due to overlap in symptoms. Although features of the clinical presentation may be useful in distinguishing bacterial from protozoan causes, they are often an unreliable indicator of the likely pathogen responsible. As with any syndromic disorder, there can be considerable overlap in symptoms caused by various agents (31). Despite efforts in recent years to educate travelers to recognize acute bacterial diarrhea (as opposed to protozoan) for purposes of self-treatment, this approach is at best empiric, and although may be suitable for travelers in remote destinations, it does not translate well to the individual with community acquired diarrhea (29).
Conventional diagnostic approaches to diarrheal disease require multiple procedures: bacterial culture, microscopy with and without stains or immunofluorescence and stool antigen tests for detection of protozoa, and for detecting viral agents, electron microscopy, or antigen-based tests. Routine clinical laboratory detection of bacterial pathogens requires the use of differential culture media, which select for the growth of certain bacteria but may fail to detect other bacteria, especially in the setting of antibiotic use. Culture methods are laborious and time consuming, with results often not available for 48 to 72 h (32). Historically, a decision to obtain a stool culture in an individual with diarrhea has often been guided by the finding of fecal leukocytes or the presence of stool lactoferrin (4, 33). Although the latter is a more sensitive predictor of a positive stool culture, using these markers to guide further diagnostic studies has been proven to be imprecise and probably unnecessary.
Microscopy has been the principal diagnostic tool in parasitology for over 350 years. The limitations of this method are that it is labor and time intensive, requires technical expertise, and lacks sensitivity and reproducibility. Multiple specimens are often required to reduce the day-to-day variability in parasite shedding (34).
When enteric viruses were identified as agents of acute diarrheal infection, commercial diagnostic tests were unavailable. A reliance on distinct characteristics of the clinical illness, often in the appropriate setting, was the standard of practice. Electron microscopical examination of stool allowed recognition of viral agents of acute diarrhea but was expensive and not widely available. Enzyme immunoassays and serologic studies are available but suffer from these limitations as well (35).
Diagnostics to determine specific microbial etiologies have advanced in the past number of years. It is now possible using culture-independent molecular techniques to rapidly and simultaneously identify a multitude of bacterial, protozoan, and viral diarrheal pathogens including some not commonly identified in clinical laboratories (36).
Diarrheal disease by definition has a broad range of potential pathogens particularly well suited for multiplex molecular testing. Several well-designed studies show that molecular testing now surpasses all other approaches for the routine diagnosis of diarrhea. Molecular diagnostic tests can provide a more comprehensive assessment of disease etiology by increasing the diagnostic yield compared with conventional diagnostic tests (Table 2). They are also faster, providing results in hours rather than days (37). The new diagnostics’ best applicability is for the clinician in practice, seeing one patient at a time rather than in the public health setting, e.g., in outbreak investigations. One potential drawback of molecular technologies is the need to predefine the particular microbes being sought. In addition the significance of an identified organism may not be clear as these molecular technologies, which involve nucleic acid amplification, are limited to our existing knowledge of a microbes’ genome and do not discriminate between viable and non-viable organisms. As a result they can detect microbes at non-pathogenic levels. Given the high rates of asymptomatic carriage of enteropathogens, this can be a considerable problem. To confound matters, further multiplex techniques are more commonly associated with increased detection of mixed infections and the relative importance of each pathogen may be unclear (38, 39, 40, 41, 42, 43, 44, 45, 46, 47).

FDA-approved laboratory tests for enteric pathogens
Before bacterial culture is discarded entirely, it is important to acknowledge that multiplex molecular diagnostics do not yield isolates that can be forwarded to public health laboratories. Specimens collected for culture-independent testing may, in some cases, be incompatible with culture because of the collection methods or media that are used for collection. And, a strict reliance on culture-independent diagnostics would limit our ability to detect new causes of diarrheal disease (26, 48, 49, 50, 51). The future may hold a combination approach where culture specimens that have yielded a positive result by culture-independent testing are then submitted to public health laboratories for subtyping and sensitivity analysis. A second specimen may need to be submitted if specimens are incompatible with cultures such as dry fecal swab specimens (52, 53, 54).
Despite an increasing number of reports worldwide of resistance to various antibiotics among bacterial enteropathogens, the clinical impact of this has yet to be manifest in a significant enough way to warrant anti-microbial susceptibility testing across the board, especially in the individual patient. In general, there appears to be a low failure rate with the use of empiric anti-microbial therapy, especially with the fluoroquinolones and macrolides (55, 56, 57, 58, 59, 60, 61, 62). Anti-microbial susceptibility testing will continue to have a role in the outbreak setting and for ongoing surveillance of local trends in resistance patterns and mechanisms (63, 64, 65).
Treatment of acute disease
Oral rehydration
Recommendation
5. The usage of balanced electrolyte rehydration over other oral rehydration options in the elderly with severe diarrhea or any traveler with cholera-like watery diarrhea is recommended. Most individuals with acute diarrhea or gastroenteritis can keep up with fluids and salt by consumption of water, juices, sports drinks, soups, and saltine crackers. (Strong recommendation, moderate level of evidence)
Summary of the evidence
One of the most significant advances in the past century was development of a balanced sodium-glucose solution that allows optimal absorption of electrolytes and water. Availability of oral rehydration solution (ORS) has reduced infant mortality in developing countries by at least 50% (66). The major value of ORS is treatment of dehydrating forms of diarrhea in infants and young children in developing countries. ORS may not reduce diarrhea and the objective of ORS therapy is not to shorten illness. In TD dehydration is not common and mortality occurs only very rarely. Among otherwise healthy people, the risk of fatality during a bout of diarrhea is most common for the elderly whether traveling or remaining in a nursing home. More than 80% of deaths in the United States associated with diarrhea occur in the elderly (67). For infants and the elderly with severe TD and in anyone who develops profuse cholera-like watery diarrhea, balanced ORS and medical evaluation are advised. In non-elderly adult travelers with diarrhea, the objectives are generally improving symptoms and getting the people back to scheduled activities. A previous study of TD management in young adults failed to identify clinical or laboratory benefit of balanced ORS therapy in patients treated with loperamide (68). For most otherwise healthy adults with TD, formal ORS is not needed as they can keep up with fluid losses by taking in salty soups, fruit juices, and carbohydrates to provide the glucose-sodium cotransport (69). Popular carbonated soft drinks provide fluids and almost no sodium or potassium, while fruit juices (e.g., apple juice) provide high levels of potassium and carbohydrate, but low levels of sodium and chicken broth is heavy in sodium (70, 71). Travelers with diarrhea should keep up with fluids and electrolytes through diet to be certain they are regularly passing urine and have moist mucous membranes.
In severe diarrhea, a balanced ORS can usually be purchased at a local pharmacy with sodium of 60–75 mEq/l and glucose of 75–90 mmol/l (72) with value in replacing fluids and salt in dehydrating forms of diarrhea as studied in infants and children. Sports drinks while not adequate alone to treat severe diarrhea can provide partial sodium and potassium replacement. More research is needed to determine the optimal composition of available fluid-salt replacement beverages for travelers (73). New developments in oral rehydration are underway, and if convenient without increasing diarrhea and without complications, they may offer advantages in the treatment of more severe forms of TD by preventing symptoms associated with mild forms of dehydration or frank dehydration in cholera-like forms of diarrhea (74).
Probiotics and prebiotics
Recommendation
6. The use of probiotics or prebiotics for treatment of acute diarrhea in adults is not recommended, except in cases of postantibiotic-associated illness. (Strong recommendation, moderate level of evidence)
Summary of the evidence
As our understanding of the importance of the human microbiome in health and disease has advanced, interest in the use of nonpathogenic bacteria and yeast, as well as nutrients that enhance the growth of favorable microbes in our bodies producing enhanced colonization resistance has also expanded (75). Probiotics are defined as live microorganisms, which, when administered in adequate amounts, confer health benefits on the host. For a microorganism to be considered a probiotic, it must exhibit non-pathogenic properties, be viable in delivery vehicles, be stable in acid and bile, adhere to target epithelial tissue, persist within the gastrointestinal tract, produce anti-microbial substances, modulate the immune system, and influence metabolic activities (76). Postulated mechanisms of action of probiotics include “colonization resistance” a barrier effect that prevents attachment or colonization of microorganisms. Probiotics supposedly act by prohibiting pathogen attachment, enhancing the immune response and by assisting in re-establishing the microflora (77). Prebiotics are non-digestible food ingredients that are fermentable in the colon and stimulate potentially health-promoting bacteria, chiefly bifidobacteria and/or lactobacilli, conferring a beneficial shift in the microbial equilibrium of the host gut flora (78). Bifidobacteria as well as lactobacilli appear to have important functions in the ecophysiology of the colonic microbiota. These organisms have been associated with an increased resistance to infection and diarrheal disease (79, 80). Prebiotics when combined with probiotics form synbiotics. Synbiotic formulations have been tested in animal models with beneficial effects on reducing adherence of pathogenic bacteria to the jejunum and colonic mucosa (81).
With respect to treatment of infectious diarrhea, it is theorized that by enhancing intestinal colonization by specific organisms there would be a reduction in the environmental niche for the offending pathogen through production of acids, hydrogen peroxide, or other anti-microbial substances, increase of mucus production, and gut barrier defense, as well as competition for nutrients or adhesion receptors, antitoxin action, and stimulation of the immune system (82). In 2010, a Cochrane systematic review was published on the topic of probiotics and treatment of intestinal infection (83). In this review, they identified 63 randomized and quasi-randomized controlled trials comparing specific probiotic agent(s) compared with a placebo or no-treatment with acute diarrhea of presumed infectious etiology. Between 1966 and 2010, 63 studies including 8,014 subjects met the eligibility criteria. Only six of these trials were among adults (84, 85, 86, 87, 88, 89). Among the pediatric studies, mostly of which were conducted among developing world populations and varied greatly with respect to settings, organisms tested and dosage, probiotics significantly reduced the duration of diarrhea (mean difference 24.8 h; 95% confidence interval (CI): 15.9–33.6 h; n=4,555, 35 trials), and the stool frequency on day 2 (mean difference 0.80 stools; 0.5–1.1; n=2,751, 20 trials). Effect sizes did not differ between studies carried out in developed or developing countries.
Table 3 describes six adult randomized controlled trials identified in the 2010 Cochrane Review and no additional randomized controlled trials have subsequently been published. These studies include two different probiotics (five studies with the single product Enterococcus LAB SF68 and one study with Sacchromyces boulardii). These studies were conducted in a variety of countries, clinical settings, and used different eligibility, treatment regimens, and primary clinical endpoints. While heterogeneity in studies is found, one product, Enterococcus LAB SF68, had one end point, diarrhea lasting greater than 4 days, which was combinable and reported in the Cochrane review. Among the four studies with similar product and end point (84, 85, 86, 87), in the probiotic arms 21/168 (12.5%) compared with 102/165 (62%) in the placebo arms had diarrhea lasting greater than 4 days. When combined, these studies achieved a 79% efficacy (relative risk: 0.21, 95% CI: 0.08–0.52) for this outcome with substantial heterogeneity (T2=0.56; χ22=10.47, d.f.=3 (P=0.01); I2=71%). However, theoretical safety concerns raised about this product limits further recommendation (90). The one study with S. boulardii did not appear to confer any advantage in the primary or secondary outcomes evaluated (89).

Randomized double-blind placebo-controlled trials evaluating probiotics in treatment effectiveness of acute diarrhea
Based on the current evidence, there are not enough studies, which would support the recommended use of any particular probiotic product for treatment in acute adult diarrhea infection. Although a statistically significant summary treatment effect was observed for Enterococcus LAB SF68, heterogeneity in results does not allow for generalization, theoretical safety concerns, and no recent studies with this product have been reported. Recommendations on use of probiotics in pediatric populations have recently been published (91).
A single study of polyphenol-based prebiotic has been described in the treatment of acute diarrhea in children and adults seeking treatment at community health centers in Managua, Nicaragua (92). No diarrhea case definition (e.g., frequency or duration) for inclusion was reported; however, exclusion critieria included those with high fever, vomiting, severe dehydration, and bloody stools. A remarkable treatment effect on mean time to last unformed stools among the treatment group compared with placebo was reported (prebiotic: 10.5 h vs. placebo: 54 h, P<0.0001). While important methodological and analytic detail are missing, and understanding of potential mechanism of action is lacking, this product may warrant additional investigation in a well-designed clinical trial.
While evidence supporting therapy of probiotics in treatment of acute diarrheal infection is lacking, and few studies addressing the effectiveness of probiotics in treatment of antibiotic-associated diarrhea (93), there is supporting evidence for the role of probiotics in prevention of acute diarrhea associated with antibiotic use (94). The pooled results among 63 randomized controlled trials across all population, setting, and probiotic types indicated a relative risk reduction of 0.58, with a number needed to treat of 13. Heterogeneity and gaps in reporting of the studies, design, population, and antibiotic associated class make clinical application of these results to the individual patient clinical care challenging. Future research is needed to support directed therapy and effectiveness among various patient populations, clinical indications, antibiotics, and probiotic strains, as well as further understanding the risk of adverse events associated with probiotic use for these indications.
Non-antibiotic therapies
Recommendation
7. Bismuth subsalicylates (BSSs) can be administered to control rates of passage of stool and may help travelers function better during bouts of mild to moderate illness. (Strong recommendation, high level of evidence)
8. In patients receiving antibiotics for TD, adjunctive loperamide therapy can be administered to decrease duration of diarrhea and increase chance for a cure. (Strong recommendation, moderate level of evidence)
Summary of the evidence
Medical treatment is not required in patients with non-severe, non-cholera-like diarrhea. Non-antibiotic anti-diarrheal drugs have been shown to reduce the number of stools passed in cases of diarrhea allowing the ill people to continue their planned schedule. The drugs with value in controlling symptoms with reduced rate of stooling are the antisecretory and antimotility drugs. Intestinal secretion is the major pathophysiologic mechanism leading to watery diarrhea in some forms of acute diarrheal infection including TD. The antisecretory drugs that have been evaluated and shown to have value for therapy in secretory forms of diarrhea are BSS (95), zaldaride maleate (96), and crofelemer (97). It is the salicylate part of BSS that has antisecretory anti-diarrheal properties (98). BSS will reduce the stools passed by ˜40% (95). Crofelemer is a cystic fibrosis transmembrane regulator chloride-channel blocker and is effective in some forms of diarrhea including TD and AIDS-associated diarrhea (99). Zaldaride is a calmodulin-inhibiting drug that has antisecretory properties related to intracellular concentrations of calcium (100). The drug significantly shortened the stools passed in subjects studied with TD compared with placebo therapy (96, 101, 102). Racecadotril, a specific enkephalinase inhibitor that prevents degradation of the endogenous antisecretory peptide neurotransmitter enkephalins that inhibit cyclic nucleotide secretory pathways without effect on gut motility (103) and has been used successfully in pediatric diarrhea (104). While racecadotril was shown to be as effective as loperamide in the treatment of acute endemic diarrhea in adults (105), this antidiarrheal drug needs to be studied further in diverse forms of diarrhea. Of the strictly antisecretory, only two agents are approved for use by the Food and Drug Administration in the United States, BSS for treatment of acute diarrhea and crofelemer for HIV-associated diarrhea. The recommended dose of BSS for therapy of acute diarrhea is 30 ml (525 mg) of liquid formulation or two tablets (263 mg per tablet) chewed well each 30–60 min not to exceed eight doses in 24 h. The drug will produce black stools and black tongues from harmless bismuth sulfide salt.
The major antimotility drugs used for therapy of acute diarrhea are loperamide and diphenoxylate. Of these, the most useful drug is loperamide, which has less central opiate effects. Another limitation of diphenoxylate is that it contains atropine, which has no antidiarrheal effectiveness and may produce objectionable side effects. Loperamide works through two mechanisms, the most important being the production of segmental contraction of the gut, which slows the intraluminal movement of fluids and allows greater absorption (106). A secondary effect appears to be inhibition of calmodulin leading to reduced mucosal secretion (107). Thus, the mechanisms of antidiarrheal effect of loperamide are indirect or direct inhibition of mucosal secretion and reduction in motility. In a comparative randomized trial in patients with TD, loperamide reduced the number of diarrheal stools passed when compared with BSS (108) and loperamide was shown to shorten diarrhea in both children (109) and adults with acute diarrhea (110). The recommended dose of loperamide for therapy for adults with diarrhea is 4 mg initially followed by 2 mg after subsequently passed watery stools not to exceed 8 mg per day. Loperamide is not given for more than 48 h. The most valuable use of loperamide in the self-treatment of TD is as a combination drug with anti-bacterial drugs where the antimotility drug quickly reduces the number of diarrhea stools passed while the antibiotic cures the enteric infection (29, 111).
A common complaint of loperamide therapy in acute diarrhea is post-treatment constipation. It is important to use the lowest dose of loperamide to provide antidiarrheal effects without the post-treatment constipation effects of the drug. Antimotility drugs have been associated with intestinal complications such as toxic dilatation of the colon or prolonged illness when used in bacterial inflammatory (112, 113), although the association is rare and if it occurs it is seen with otherwise untreated diarrhea caused by the highly inflammatory bacterial pathogens. When inflammatory forms of colitis are also treated with anti-microbial drugs, this potentiation is very unlikely to occur (113).
Adsorbent drugs such as kaolin, pectin, charcoal, and attapulgite do have an effect on form of stools passed, but the number of stools passed and duration of post-treatment diarrhea are not shortened (114, 115) and are not recommended.
Antibiotic therapy
Recommendation
9. The evidence does not support empiric anti-microbial therapy for routine acute diarrheal infection, except in cases of TD where the likelihood of bacterial pathogens is high enough to justify the potential side effects of antibiotics. (Strong recommendation, high level of evidence)
10. Use of antibiotics for community-acquired diarrhea should be discouraged as epidemiological studies suggest that most community-acquired diarrhea is viral in origin (norovirus, rotavirus, and adenovirus) and is not shortened by the use of antibiotics. (Strong recommendation, very low level evidence)
Summary of evidence
The evidence for the use of anti-microbial therapy is strongly supported for cases of TD (Table 4 lists acceptable regimens). Numerous studies have demonstrated that antibiotics shorten the overall duration of moderate-to-severe TD to a little over 24 h (116). The primary efficacy parameter in most clinical trials has been the time from initiation of therapy until the last unformed stool is passed (117). Anti-bacterial drugs have been shown to reduce initiation of therapy until the last unformed stool is passed in cases of TD by 1–3 days compared with no therapy or placebo (118, 119, 120, 121), and combination of an antibiotic with loperamide further shortens duration of illness (111). Fluoroquinolones such as ciprofloxacin or levofloxacin have been the primary antibiotics of choice for most destinations (119, 120, 122), although growing resistance to this class of antibiotics may change this (123, 124, 125). In addition, there is evidence that most Campylobacter are fluoroquinolone resistant and the use of macrolides such as azithromycin for treatment is recommended (126). Azithromycin was shown to be more effective than ciprofloxacin for all cases of TD in travelers to Thailand, probably because of the high prevalence of Campylobacter in this region (127).

Acute diarrhea antibiotic treatment recommendations
A review of nine randomized clinical trials and one Cochrane review assessing fluoroquinolone use for the treatment of TD (116, 119, 122, 128, 129, 130, 131) found overall reductions in diarrhea duration compared with placebo and evidence from these studies showed no serious harm associated with fluoroquinolone use; however, the literature on the use of flouroquinolones in all settings has demonstrated risks of development of Clostridium difficile infection and risks for tendonopathies and arthropathies (132). For all antibiotics, either single-dose therapy or treatment for up to 3 days is usually sufficient to allow resolution of symptoms. Studies show that once daily therapy is as effective as 3-day therapies for TD due to noninvasive pathogens, which comprise the majority of cases (120, 121). A 3-day therapy is recommended for patients presenting with fever or dysentery. Enteric infection by Shigella dysenteriae appears to be an exception, insofar as 5 days of therapy appears to be superior to single-dose or 3-day therapy (125). With increasing resistance to ampicillin and trimethoprim/sulfamethoxazole, azithromycin has been the treatment of choice (133, 134). Recently, however, Shigella sonnei has been found to have reduced susceptibility to azithromycin among isolates in the United States (61).
Although no studies looked at the efficacy of azithromycin vs. placebo, there were four randomized controlled trials that compared azithromycin to the flouroquinolones in the treatment of TD (118, 127, 135, 136). No difference was noted in efficacy between the two treatment groups. Among adult student travelers to Mexico, a single dose 1,000 mg azithromycin was comparable to levofloxacin 500 mg in shortening the duration of illness (22.3 vs. 21.5 h) (118). Three trials demonstrate that azithromycin was as effective as a fluoroquinolone in the treatment of TD occurring in Thailand or Mexico (118, 125, 127). Azithromycin was also shown to be active in the treatment of diarrhea caused by Campylobacter including fluoroquinolone-resistant strains (125, 137). Azithromycin is effective against Shigella spp., as well as noninvasive diarrheagenic Escherichia coli (137, 138). Looked at as a whole, these studies suggest that azithromycin is as effective as the flouroquinolones in providing relief from TD. Anti-microbial resistance patterns for azithromycin have been studied but results are inconclusive. One study showed that azithromycin had high activity against TD pathogens but another suggested that concentrations needed to inhibit diarrheagenic E. coli have been increasing over the past decades. (26) In vitro studies showed increasing resistance among Campylobacter isolates in Nepal and Thailand but clinical failures have not been reported (139).
Rifaximin, a non-absorbable rifamycin-derived antibiotic, has been shown to be effective against diarrheagenic E. coli, which appear to be the most common bacterial pathogens in the Western Hemisphere (140). In two studies evaluating rifaximin compared with placebo, rifaximin was associated with a higher percentage of travelers cured. A follow-up study carried out on a subset of patients with diarrhea because of EAEC showed the 200 mg dose administered three times a day was more effective than placebo in decreasing median initiation of therapy until the last unformed stool is passed (22 vs. 72 h) (141). Two additional studies directly compared rifaximin with ciprofloxacin. There was no significant difference with respect to cure or treatment failure (142, 143). Another study failed to demonstrate overall advantage when ciprofloxacin was compared with rifaximin in TD in Mexico, Guatemala, and India. However, a subgroup with invasive illness showed a reduced benefit following treatment with rifaximin (131).
While individual self-treatment of TD among travelers has been common since the late 1980s, there are a few microbe-specific concerns with the use of empiric anti-bacterial therapy of TD. The first is that anti-bacterial drugs appear to complicate enteric disease caused by Shiga-like toxin-producing E. coli by increasing the risk of hemolytic uremic syndrome. Although this may occur more commonly in children, a meta-analysis did not show an association between anti-microbial therapy in adult patients with hemorrhagic colitis due to E. coli 0157:H7 and the subsequent development of hemolytic uremic syndrome (144). Another theoretical concern with antibiotic use is that for non-typhoidal Salmonella strains, there may be prolonged intestinal carriage. A meta-analysis showed that antibiotic therapy does not appear to reduce the length of illness in immunocompetent adults and increases the period during which Salmonella was detected in stool (144). This however would not necessarily be an argument against antibiotic use as short-term carriage appears to be of limited clinical significance to those who are affected (145).
Another perhaps more legitimate concern is that treatment with antibiotics will modify the microbiota. This may result in the development of C. difficile-associated diarrhea or colitis (132, 145). A recent publication reported patients who developed C. difficile colitis following treatment with ciprofloxacin (146). However, this does not appear to be a common adverse outcome associated with treated TD. We are becoming increasingly aware that changes in an individual’s gut microbiota may be associated with international travel to certain destinations. In a recent study, it was shown that antibiotic use for self-treatment of TD increases a traveler’s risk of colonization by resistant bacteria namely extended spectrum β-lactamase-producing Enterobacteriaceae and carbapenemase-producing Enterobacteriaceae. In this study, travel itself was associated with a 21% rate of colonization by extended spectrum β-lactamase-producing Enterobacteriacceae, but remarkably 80% of travelers who self-medicated with antibiotics became colonized with these microorganisms, raising the possibility that this might contribute to the spread of resistant intestinal bacteria to the population at large in developed countries (147). Changes in one’s gut microbiota might have consequences with respect to an individual’s susceptibility to infection or postinfectious consequences of intestinal infection as well, but this is speculative at present (148). At present, the risk of acquired extended spectrum β-lactamase on the individual and community vs. the potential negative consequences of untreated TD has raised awareness and interest in the development of more data to inform management decisions.
The evidence is strong for anti-microbial treatment of specific parasitic causes of acute diarrheal infection such as metronidazole, tinidazole, or nitazoxanide for Giardia infections, metronidazole or tinidazole for Entameba histolytica, nitazoxanide for Cryptosporidiosis, trimethoprim/sulfamethoxasole for Cyclosporiasis or Cystisosporiasis, albendazole for Enterocyotzooan bienusi, or iodoquinol for Diemtameba fragilis (149, 150, 151, 152, 153, 154, 155). With the advent of new molecular diagnostics, more specific diagnoses including parasitic etiologies may be made more promptly, guiding the targeted use of anti-microbial therapy (both agent and duration of treatment) to match a specific pathogen.
Evaluation of persisting symptoms
Recommendations
11. Serological and clinical lab testing in individuals with persistent diarrheal symptoms (between 14 and 30 days) is not recommended. (Strong recommendation, very low level of evidence)
12. Endoscopic evaluation is not recommended in individuals with persisting symptoms (between 14 and 30 days) and negative stool work-up. (Strong recommendation, very low level of evidence)
Summary of evidence
In the evaluation of the patient with persistent symptoms, a thorough and directed history is essential. Relevant questions would include travel history, the nature of the initial symptoms, onset (sudden or gradual), duration, frequency and characteristics of bowel movements (particularly the presence of blood or mucus), stool volume, tenesmus, pattern, association with particular foods, use of antibiotics, and the presence or absence of other associated symptoms such as nausea, vomiting, incontinence, fever, and weight loss. The answers to these questions may direct further investigations (156).
Among patients with persistent symptoms (between 14 and 30 days), the role of clinical laboratory studies and endoscopy is uncertain and should be dictated by clinical suspicion and disease severity, within the context of most likely etiologies. An initial diagnostic evaluation in the patient with persistent symptoms should include tests for the presence of microbial pathogens. Although stool culture and microscopy remain the initial diagnostic tests, they both suffer from limitations that may be addressed by newer diagnostic methods. Even some of the newer methods, such as enzyme-linked immunoassays and direct immunofluorescence staining, which increase sensitivity, may not be able to distinguish, e.g., between the pathogen Entamoeba histolytica and a non-pathogenic but microscopically indistinguishable Entamoeba dispar. (157). Singleplex and multiplex PCR assays for the detection of enteric microbial pathogens are more sensitive than culture, microscopy, or antigen detection (158, 159, 160). In one study describing a real-time PCR assay designed to detect Giardia intestinalis, the lower limit of detection was as little as 102 spores per ml of stool as opposed to microscopy, which required >106 spores per ml of stool (161).7 One study showed using PCR methods resulted in a 22-fold increase in the detection of Cryptosporidium and Giardia compared with conventional microscopy (162). Colonoscopy has been considered in the evaluation of the patient with persistent diarrhea. In a recent study looking at the diagnostic value of endoscopy for the diagnosis of giardiasis or other intestinal diseases in patients with persistent diarrhea returning from tropical or subtropical areas, lower endoscopy (colonoscopy or sigmoidoscopy) yielded relevant diagnoses more often than upper endoscopy (163). This study, however, suffers from a small sample size insofar as only 31 patients with persistent diarrhea were examined and thus the additional value of such procedures cannot be recommended. In certain clinical situations such as postantibiotic or hospital-acquired gastrointestinal illness, testing for Clostridium difficile may be recommended, as well as additional serologic and clinical laboratory testing including a complete blood count, which may be helpful in informing an infectious cause in the absence of revealing stool studies.
While not considered in these guidelines, the work-up of chronic diarrhea is briefly considered and should include the differential diagnoses such as celiac disease, Crohn’s disease, eosinophilic gastroenteritis, and Whipple’s disease. Gastrointestinal endoscopy and relevant serological assays may contribute to the diagnosis and management if sustained or progressive weight loss is a prominent feature, and upper endoscopy may be considered, especially if empiric therapy and symptomatic measures have not helped. Mucosal biopsies are recommended even when the endoscopic appearance is normal. The diagnostic yield of colonoscopy in patients ranges from 7 to 32%, with IBD and microscopic colitis being the most common diagnoses (164, 165, 166, 167, 168, 169). It has also been seen that colonoscopy yields a noninfectious diagnosis more often than upper endoscopy (170, 171, 172). A review of 18 primary studies looking at the diagnostic value of colonoscopy in patients with chronic diarrhea, as well as a review of nine published guidelines provides the basis for a colonoscopy recommendation in such patients (165, 167, 168, 173, 174, 175, 176, 177, 178, 179, 180, 181, 182, 183, 184, 185, 186).
In the situation of chronic diarrhea and abdominal symptoms occurring after a bout of infectious diarrhea, a diagnosis of postinfectious irritable bowel syndrome must be considered (187). Postinfectious irritable bowel syndrome requires a paradigm shift: an external event, in this case a gastrointestinal infection, leads to prolonged and permanent changes in gastrointestinal function, which do not appear to be directly mediated by the persistence of an infectious agent. There appears to be a physiologic basis for the apparent failure to downregulate intestinal inflammation but there are no commercially available serologic or other diagnostic tests to confirm and the diagnosis rests on using conventional criteria such as Rome III in patients who have been sick with gastroenteritis or TD.
Prevention
Counseling
Recommendations
13. Patient level counseling on prevention of acute enteric infection is not routinely recommended but may be considered in the individual or close-contacts of the individual who is at high risk for complications. (Conditional, very low level of evidence)
14. Individuals should undergo pretravel counseling regarding high risk food/beverage avoidance to prevent TD. (Conditional, very low level of evidence)
Summary of evidence
Non-travel setting: One in six US citizens get sick from a foodborne illness each year, and a majority of these illness will be from contaminated food consumed in the United States (e.g., non-travel associated) (1, 2). Food safety is a major public health effort that involves multiple Federal, State, and local agencies including the Food and Drug Administration, US Department of Agriculture, US Food Inspection Service, and state and local health departments, all of which focus on the potential risks for large outbreaks associated with centralization of food processing and reliance on imported foods. However, to reduce the burden of disease the responsibility of foodborne prevention must not only include the producers on the farm, packaging industries, stores, and restaurants but also penetrate down to the individuals in the home who are buying and preparing food—the last step in the chain of foodborne illness prevention.
The intervention of improving food preparation in the home has not been systematically studied. The Centers for Disease Control has recently responded through launching a new consumer food safety campaign to educate the public on the simple message of clean, separate, cook, chill, and report. No recommendations on counseling by providers have been provided. No recommendations on counseling by providers have been recommended. However, for vulnerable patient populations who are at increased risk for severe disease and complications associated with acute foodborne illness, including pregnant women, elderly, and those with immune deficiency due to HIV or immunotherapeutic, situational individual patient level counseling may be appropriate.
Traveler setting: In the realm of travel medicine, Shlim reviewed the evidence for the effectiveness of personal hygiene precautions in prevention of TD (188). In the eight studies identified in this 2005 review, seven found no correlation between the types of food selected by the traveler and the risk of acquiring traveler’s diarrhea, whereas one showed a correlation between a few dietary lapses. The summary from this review provides the basis for current recommendations where it was stated, “The sum total of these errors leads to abundant opportunities for the spread of enteric pathogens, whether from employees’ hands, flies, or contaminated meat and produce, with ample time available for bacterial growth to reach infective levels. One could postulate that “boil it, cook it, peel it, or forget it” would be good advice to someone who was purchasing and preparing their own food in a sanitized kitchen but that it is inadequate for travelers faced with the multiplicity of hygienic errors found in the kitchens of many destination countries”.
Subsequent to this review there have been few studies reported on this topic. A recent report among travelers who attended a travel clinic before travel (‘exposed’) and travelers to similar regions but did not attend travel clinic (‘non-exposed’) was reported (189). In this study, 13 (4.3%) of those interviewed reported drinking unsafe water and this proportion was similar in those who attended or did not attend travel clinic before travel (exposed (n=7/150, 4.6%) and non-exposed subjects (n=6/150; 4%) (P=0.78)). Forty-five (15%) of enrolled subjects ate some food with elevated risk of traveler’s diarrhea (such as raw fruit or vegetables, drink with ice or ice cream); this proportion was higher in the non-exposed people (n=36/150; 24%) than in the people attending the Travel Clinic (n=9/150; 6%) (P<0.0001). Fifty (16.7%) reported diarrhea or gastrointestinal symptoms, 9 (6%) in the group of exposed subjects and 41 (27.3%) in the non-exposed group (P<0.0001), suggesting some effect of pretravel counseling, although there could have been other factors related to the self-selection of exposed (more cautious given their seeking out of pretravel counseling) and non-exposed travelers, which could explain these differences.
In summary, the evidence of counseling effectiveness on TD risk reduction related to food and water indiscretion is mixed and lacks recent high-quality studies.
Hand washing
Recommendation
15. Frequent and effective hand washing and alcohol-based hand sanitizers are of limited value in preventing most forms of traveler’s diarrhea but may be useful where low-dose pathogens are responsible for the illness as for an example during a cruise ship outbreak of norovirus infection, institutional outbreak, or in endemic diarrhea prevention. (Conditional recommendation, low level of evidence)
Summary of evidence
Traveler setting: The evidence of hand washing and use of alcohol-based hand sanitizers in preventing TD is mixed. Theoretically, they would be most effective in prevention of enteric infection caused by pathogens causing illness at low inoculum doses. Enteric pathogens can be divided into three categories based on expected dose necessary to cause diarrhea. The most contagious enteric pathogens are noroviruses and Shigella strains (190) because of low inoculum requirements plus stability in the environment (191). Hand washing should be effective in reducing these highly communicable pathogens and should be aggressively pursued in settings where one of these is likely to occur, e.g., during cruise-ship travel or in a community or institutional outbreak due to one of these pathogens.
The expected dose for the diarrheagenic E. coli strains, the most common causes of TD, is high in the level of one million bacteria or higher (192, 193) with the infections nearly always a result of ingestion of contaminated foods where food has been improperly handled allowing propagation of the pathogen to diarrhea-causing levels. Effective hand washing or regular use of alcohol-based hand sanitizers could well be useful in preventing TD if thoroughly pursued by persons preparing food eaten by other travelers, but is unlikely to impact when done by the person consuming the contaminated food.
For cruise travelers regular hand washing can be useful in case there is apparent or inapparent transmission of norovirus infection. Alcohol-based hand sanitizers often have anti-viral properties (194), although in one study hand washing with soap and water was effective in removing norovirus from hands, while alcohol-based hand sanitizers were not (195). In a retrospective survey of protective measures against TD, regular use of alcohol hand sanitizers did not appear to offer any protection against either diarrhea or respiratory tract infection in travelers (196). Again, this lack of prevention of TD probably relates to the high inoculum requirements of the common forms of infection. This is in contrast to the established value of hand washing in preventing endemic pediatric diarrhea in developing regions where lower inoculum pathogens are common (197, 198). In developing regions the presence of soap in homes is associated with reduced diarrhea rates in local populations living in unhygienic areas (199). Alcohol-based hand disinfectant use in a public setting in Germany did provide protection against respiratory and diarrheal illness in a randomized study in local non-traveling inhabitants (200). Hygiene including hand washing undoubtedly has a greater effect in preventing diarrhea in wilderness backpackers (201) who may have exposures more resembling endemic settings in the developing world than those seen with typical travelers staying in clean hotels.
Prophylaxis
Recommendations
16. Bismuth subsalicylates have moderate effectiveness and may be considered for travelers who do not have any contraindications to use and can adhere to the frequent dosing requirements. (Strong recommendation, high level of evidence)
17. Probiotics, prebiotics, and synbiotics for prevention of traveler’s diarrhea are not recommended. (Conditional recommendation, low level of evidence)
18. Antibiotic chemoprophylaxis has moderate to good effectiveness and may be considered in high-risk groups for short-term use. (Strong recommendation, high level of evidence)
Summary of evidence
Traveler setting: Prevention of TD is challenging because of the ubiquitous exposures to individuals through contaminated food, water, and generally unhygienic conditions among much of the developing world. Travelers are frequently counseled on preventive risk behaviors, but despite a traveler’s best attention to such recommendations, evidence is lacking that such precautions have any protective effect (188). Although vaccines for many of the agents commonly associated with TD are under development, these are considered a long-term solution and might likely suffer from the lack of utilization as has been seen with most travel-associated vaccines (202, 203, 204, 205, 206). Alternative primary prevention strategies such as BSS, probiotics, and antibiotics have been evaluated and are considered here.
Bismuth subsalicylate
BSS has been shown in several studies to reduce the frequency of TD when used during period of risk for 3 weeks (207, 208, 209). While the salicylate portion of the drug provides antidiarrheal effects, it is the bismuth moiety that is active when the molecule is used for chemoprophylaxis (210). BSS and the bismuth reaction products found in the gut have dose-responsive activity against bacteria (211) and anti-viral properties (212). The drug provides at least 60% protection in a dose of 2.1 g per day (207, 208). The recommended dose of BSS for TD prevention is two tablets four daily doses at mealtimes and at bedtime. Both the dose and the interval of administration appear to be important as 2.1 and 1.05 g given two times a day led to reduced levels of protection, 41% and 35%, respectively (209). The chemoprophylactic dose of BSS leads to important absorption of salicylate and should not be used when other salicylates are being taken. BSS does not have the damaging effects on gastric mucosa as acetyl salicylic acid effects and, in fact, has intestinal mucosa-cytoprotective effects (213, 214).
BSS use has been shown to reduce the occurrence of TD if taken in proper daily dose for up to 3 weeks. Most authorities recommend that chemoprophylaxis could be used for trips up to 2 weeks (215). Chemoprophylaxis should not be used for longer trips. Future travelers planning to use BSS chemoprophylaxis need to be warned that during administration of the drug their stools and tongues will turn black and that this harmless bismuth sulfide salt is of no medical concern. Persons with underlying inflammatory bowel disease or HIV infection should not receive BSS because of the fear of excessive absorption of this generally poorly absorbed bismuth compound leading to bismuth encephalopathy (216).
Probiotic/prebiotic/synbiotics
The use of probiotics, prebiotics, and synbiotics to prevent acute diarrheal infection is an appealing concept because of their ease of use and relative safety. The data, however, supporting their use in preventing infectious diarrhea is not consistently strong and at this point we do not recommend them for this purpose
The preventive role of probiotics, prebiotics, and synbiotics in acute diarrheal infection in adults is limited to studies in prospective travelers (217, 218, 219, 220, 221, 222, 223, 224, 225, 226). There are no published studies in the setting of community-acquired diarrhea, in the outbreak setting for example. Available studies suffer from variability in age groups, setting, causes of acute diarrhea, and probiotic strains. Although most of the trials are of adequate quality, limitations include short follow-up and not estimating person-time analysis. There were also large variations in the dosage of probiotics, frequency of administration, and formulations used. Further variation was seen with regard to timing and administration of these preparations relative to a number of factors including travel and concurrent treatment with anti-microbials (217). Although two meta-analyses suggest a marginal benefit of probiotics in prevention of TD, both suggest there is insufficient evidence for extrapolation to global recommendations for their use (217, 218).
Probiotics
In the past three decades, trials investigating the effects of probiotics in the prevention of TD have demonstrated varying results (219). In one of the earlier studies, Enterococcus faecium did not prevent TD. In a study by the same group, Saccharomyces boulardii given to 3,000 Austrian travelers in a placebo-controlled manner resulted in a clinically modest dose-dependent benefit in TD prevention, effects were most impressive in travelers to North Africa and Turkey (220). In a study of 756 Finnish travelers to two separate destinations in Turkey, a 41% diarrhea attack rate was noted in the Lactobacillus GG group vs. 46.5% in the placebo group, a very modest difference. However, the rate of protection was 39.5% at one location and almost nil at the other location (221). In a US study of 245 travelers to various destinations those taking Lactobacillus GG experienced a 3.9% incidence of diarrhea per day at risk vs. 7.4% in the placebo group. Using this novel approach to protective efficacy, they calculated a protection rate of 47% (222). Lactobacillus bulgaricus as well as Lactobacillus fermentum preparations were found to be ineffective in preventing TD (223, 224) and there was no beneficial effect seen with a nonviable formulation of Lactobacillus acidophilus in the prevention of TD in a randomized placebo-controlled trial in travelers to West Africa and other destinations (227).
Prebiotics and synbiotics
Early work showed the prebiotic Lactulose reduced intestinal carriage of Shigella but was ineffective in treating Shigella infections (228). In a small study of 42 adult patients traveling to tropical countries (22 in the study group, 20 in the placebo group), the use of sodium butyrate and short-chain fatty acids as a prebiotic was evaluated for the prevention of TD (229). Noted was a significant reduction in the occurrence of TD in the prebiotic group (4.5%) vs. 40% in the placebo group. Sodium butyrate has been established in animal studies as a regulator of the intestinal environment. Limitations of the study included sample size and lack of diversity among the travelers. A double-blind, placebo-controlled trial of a novel galacto-oligosaccharide mixture in 159 healthy travelers to countries of low and high risk for TD showed a significant reduction in diarrhea in the prebiotic group as compared with those who consumed placebo (maltodextrin) (225). This particular formulation was studied because of earlier work showing this agent increased bifidobacferium numbers in the colonic content of piglets and inhibited the attachment of enterohepatic E. coli and Salmonella enterica Typhimurium to HT29 cells in vitro (230). A randomized, double-blind, placebo-controlled trial of an oral synbiotic AKSB, a combination of two probiotics (Enterococcus faecium and S. cervisiae) and a prebiotic (fructo-oligosaccharide), failed to show benefit (226).
For probiotics, prebiotics, and synbiotics alike the challenge has been to find the right formulation or combination for the right condition or individual. Mirroring the use of these agents in other gastrointestinal diseases, a more thorough knowledge of the host microbiome might be necessary before appropriate trials can be designed using specific agents for prevention.
Antibiotics
Anti-microbial prophylaxis has been considered an option to prevent infection. In 1985 issues surrounding prophylaxis were debated during an NIH-sponsored consensus meeting, which concluded that routine antibiotic chemoprophylaxis should not be used because of concerns about the development of antibiotic resistance, the demonstrated efficacy of empiric therapy after the development of symptoms, and the potential for unnecessary side effects (231). Since that meeting, studies that have examined the cost benefit of chemoprophylaxis for the prevention of TD have recommended against prophylaxis except in high-risk groups (232, 233). While debate continues, the standard practice and recommendation has remained unchanged for 20 years (234, 235, 236).
Two recent developments are challenging the general recommendation against use of chemoprophylaxis. First, postinfectious irritable bowel syndrome has been recognized as an important chronic health consequence, occurring in a sizeable proportion of those who experience an episode of TD, particularly among those with bacterial infection and a more severe clinical presentation (237, 238, 239). Second, rifaximin, a non-absorbable antibiotic, has been developed and may provide a safer alternative for prophylaxis than fluoroquinolones, which are known to be quite effective but may have an unacceptable safety profile. The high volume of international travel and, consequently, the high number of people at risk for acquiring TD, postinfectious irritable bowel syndrome and other postinfectious chronic health conditions, creates a potentially large burden of illness that could be prevented with the use of safe and effective chemoprophylaxis. However, safety concerns associated with antibiotic use, of any class, is an important consideration.
A recent systematic review summarized several studies showing a comparative advantage of antibiotic chemoprophylaxis for the prevention of TD (240). Four rifaximin studies included in the meta-analysis had a total of 604 subjects. One of those studies (DuPont et al. (241)) had three treatment arms (rifaximin 200 mg dosed once, two and three times a day) and one control arm (placebo dosed three times a day). There was no observed significant difference of risk reduction among dosing regimens in the Dupont et al. study, and the overall pooled DerSimonian and Laird effect (relative risk) estimate for all studies combined was 0.33 (95% CI: 0.24–0.45), equating to a protective efficacy of 67% (95% CI: 55–76%) favoring chemoprophylaxis (heterogeneity χ2=3.09, P=0.377; I2=3.1%). In terms of absolute risk reduction, pooled DerSimonian and Laird summary estimates found that rifaximin chemoprophylaxis decreased TD attack rates by a mean of 22.1% (95% CI: 6.3–37.9%) equating to a number needed to treat of 4.5 (95% CI: 2.6–15.9). With respect to rifaximin chemoprophylaxis, two studies (Armstrong et al. (242) and Flores et al. (243)) did not show that chemoprophylaxis with rifaximin reached a statistically significant difference in preventing TD compared with placebo (242, 243). In both studies the incidence of TD in the control group was relatively low (8/48 or 17% and 9/47 or 19%, respectively), which could have explained the findings given sample size calculations were based on the expected incidence of TD to be 40%, and thus recruitment may have been too small to detect the true effect of rifaximin in preventing TD. Most recently, an effectiveness study by Zanger et al. (244) reported moderate protection with rifaximin for up to 28 days to the South and Southeast Asian regions (244). Efficacy was noted to be higher in travelers to countries in South Asia (65%, 95% CI: 15–77) compared with Southeast Asia, which is likely attributed to differential (invasive) pathogen distributions (no microbiology was conducted in the study). However, a study by Taylor et al. (245) suggests that rifaximin may be effective against shigellosis, which is a common invasive TD pathogen (and also associated with chronic health complications) (246). There were no serious adverse drug-associated safety adverse events reported among these published studies.
While no recent studies have been conducted, floroquinolones consistently demonstrate a higher effectiveness in the prevention of TD with a summary pooled estimate of 88% (95% CI: 80–93%) protective efficacy (240). The emergence of fluoroquinolone resistance to commonly encountered TD pathogens may be a factor today if these studies were replicated (139, 247, 248). Furthermore, relative to rifaximin, the safety profile for floroquinolones is less favorable given the association with tendonopathies and the systemic broad-spectrum nature of this antibiotic with attendant pressures on systemic drug-resistant pathogens of importance (132).
The evidence to date suggests moderate to good efficacy of rifaximin and floroquinolones for chemoprophylaxis. However, until such studies are carried out, which adequately assess the risk and benefits of this strategy in reduction of acute and chronic consequences while balance the negative consequences of antibiotic use, recommendations for use in the traveler setting should be restrictive and used in short durations. The traveler who is at high risk for TD and susceptible to potentially serious health consequences, or whose illness may critically impact the intended purpose of travel, may benefit from antibiotic chemoprophylaxis.
ACKNOWLEDGMENTS
This guideline was produced in collaboration with the Practice Parameters Committee of the American College of Gastroenterology. The Committee gives special thanks to Ganesh R. Veerappan, who served as guideline monitor for this document. We thank the Cornell University reference librarian, Kevin Pain, for his assistance and expertise in conducting the systematic review of the literature and providing articles. We also are grateful to Lauren Gerson for her support and direction in the development of this guideline.
Disclaimer
The views expressed in this article do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the US Government. This is a partial US Government work. There are no restrictions on its use.
Appendix 1
Search Strategy
Ovid MEDLINE(R) 1946 to February Week 3 2015, searched on 18 February 2015.
1. Diarrhea/
2. Acute Disease/
3. 1 and 2
4. Dysentery/
5. Gastroenteritis/
6. 4 or 5
7. 1 and 6
8. 2 and 7
9. “acute”.tw.
10. 7 and 9
11. 8 or 10
12. 3 or 11
13. Acute infectious diarrh*.tw.
14. Travel* diarrh*.tw.
15. Postinfectious irritable bowel syndrome.tw.
16. Acute enteric infection.tw.
17. Acute infectious gastroenteritis.tw.
18. Infectious diarrh*.tw.
19. (Acute or chronic or severe or persistent).tw.
20. 18 and 19
21. or/13–17
22. 12 or 20 or 21
23. Limit 22 to “all child (0 to 18 years)”
24. 22 not 23
25. Limit 24 to case reports
26. 24 not 25
27. Limit 26 to english language
28. Limit 27 to last 10 years
29. Limit 28 to humans
Ovid MEDLINE(R) In-Process and Other Non-Indexed Citations, searched on 18 February 2015.
1. Acute infectious diarrh*.tw.
2. Travel* diarrh*.tw.
3. Postinfectious irritable bowel syndrome.tw.
4. Acute enteric infection.tw.
5. Acute infectious gastroenteritis.tw.
6. Infectious diarrh*.tw.
7. (Acute or chronic or severe or persistent).tw.
8. 6 and 7
9. or/1–5
10. 8 or 9
11. (Child* or infan* or p?ediatric).tw.
12. 10 not 11
13. Limit 12 to english language
14. Limit 13 to last 10 years
Embase 1974 to 2015 February 18 (Ovid), searched on 18 February 2015
1. Acute diarrhea/
2. Infectious diarrhea/
3. Dysentery/
4. Acute gastroenteritis/
5. 1 or 2
6. 3 or 4
7. 5 and 6
8. Acute infectious diarrh*.tw.
9. Travel* diarrh*.tw.
10. Post infectious irritable bowel syndrome.tw.
11. Acute enteric infection.tw.
12. Acute infectious gastroenteritis.tw.
13. Infectious diarrh*.tw.
14. (Acute or chronic or severe or persistent).tw.
15. 13 and 14
16. or/8–12
17. 5 or 7 or 15 or 16
18. Limit 17 to (embryo or infant or child or preschool child <1 to 6 years> or school child <7 to 12 years> or adolescent <13 to 17 years>)
19. 17 not 18
20. Limit 19 to english language
21. Limit 20 to exclude medline journals
22. Limit 21 to last 10 years
23. “case report”.mp.
24. 22 not 23
25. Limit 24 to human
26. (Child* or infan* or p?ediatric).tw.
27. 25 not 26
REFERENCES