April 09, 2024
2 min read
April 09, 2024
2 min read
Triennial blood-based screening for colorectal cancer was not cost-effective compared with existing screening modalities such as colonoscopy, fecal immunochemical test and stool DNA testing, according to microsimulation model projections.
“The performance characteristics of blood-based screening tests, especially for the detection of advanced adenomas, may render blood-based tests less effective than current guideline-endorsed modalities,” Rosita van den Puttelaar, MSc, of the department of public health at Erasmus University Medical Center, and colleagues wrote in Gastroenterology. “Despite this, CMS issued a coverage decision that states that triennial blood-based screening tests for individuals aged 50 to 85 years will be covered if the blood test meets a minimum performance sensitivity of 74% for detection of CRC and specificity of 90%.”

Using three independently developed microsimulation models (MISCAN-Colon, CRC-SPIN and SimCRC) from the U.S. National Cancer Institute’s Cancer Intervention and Surveillance Modeling Network, researchers investigated the efficacy and cost-effectiveness of a hypothetical triennial blood-based screening test vs. no screening, as well as annual fecal immunochemical test (FIT), triennial stool DNA test combined with FIT (sDNA-FIT) and colonoscopy every 10 years.
The models generated a cohort of 10 million individuals aged 45 to 75 years at average risk for CRC, for which researchers simulated screening, follow-up and surveillance consistent with recommendations.
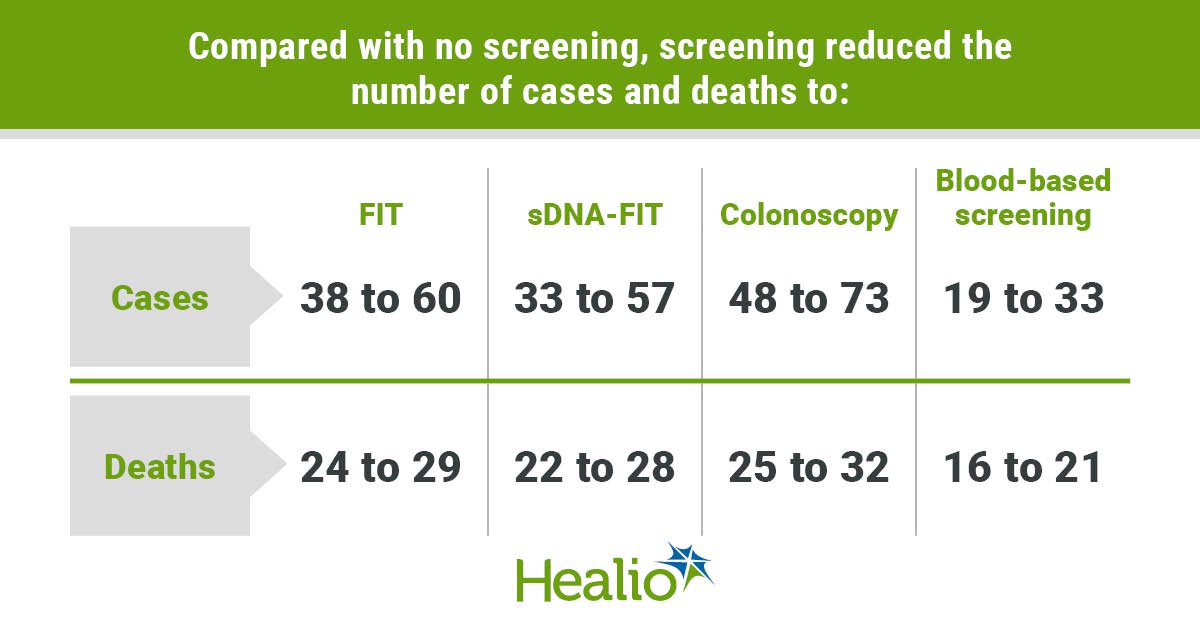
According to results, the models predicted 77 to 88 cases of CRC and 32 to 36 deaths per 1,000 people without screening, at a cost of $5.3 to $5.8 million on CRC treatment. Compared with no screening, screening reduced the number of cases and deaths to 38 to 60 and 24 to 29, respectively, with FIT; 33 to 57 and 22 to 28 with sDNA-FIT; 48 to 73 and 25 to 32 with colonoscopy; and 19 to 33 and 16 to 21 with blood-based screening.
While blood-based screening was cost-effective with an additional cost of $25,600 to $43,700 per quality-adjusted life-year (QALY) gained compared with no screening, it was not cost-effective compared with the other screening strategies. Compared with FIT, blood-based screening resulted in 39 to 68 fewer QALYs per 1,000 and increased costs by $4 to $4.8 million, with similar trends reported when compared with colonoscopy (45-84 fewer QALYs; increase of $2.3-$3.4 million) and sDNA-FIT (26-59 fewer QALYs; increase of $1.3-$2.1 million).
Researchers also noted that even if blood-based screening uptake was 20 percentage points higher than FIT or colonoscopy uptake, it still resulted in 5 to 24 fewer QALYs and a $3.2 to $3.5 cost increase vs. FIT and 10 to 34 fewer QALYs and a $2.2 to $2.6 cost increase vs. colonoscopy.
“Blood-based screening test with performance characteristics that meet the CMS coverage criteria is cost-effective compared to no screening,” van den Puttelaar and colleagues wrote. “However, blood-based screening with these performance criteria was estimated to be less effective and more costly than the currently recommended FIT, sDNA-FIT and colonoscopy screening strategies.”





