ACG Clinical Guideline: Management of Crohn’s Disease in Adu… : Official journal of the American College of Gastroenterology

INTRODUCTION
Crohn’s disease has been increasing in incidence and prevalence worldwide. At the same time, the number of therapeutic options is rapidly increasing. The purpose of this guideline is to review Crohn’s disease clinical features and natural history, diagnostics, and therapeutic interventions.
To prepare this guideline, literature searches on the different areas were conducted using Ovid MEDLINE from 1946 to 2018, EMBASE from 1988 to 2018, and SCOPUS from 1980 to 2018. The major terms that were searched were Crohn’s disease, inflammatory bowel diseases (IBD), regional ileitis, and regional enteritis. These were translated into EMTREE controlled vocabulary as enteritis and Crohn’s disease. The remainder of the search included key words related to the subject area that included clinical features, natural history, diagnosis, biomarkers, treatment, and therapy. For each of the therapeutic sections, key words included the individual drug names. The results used for analysis were limited to primary clinical trials, meta-analyses, systematic reviews, and prior guidelines. Where there were limited data, abstracts were used. In many areas reviewed, there were not available clinical trial data, and these areas are discussed as summary statements rather than GRADE statements.
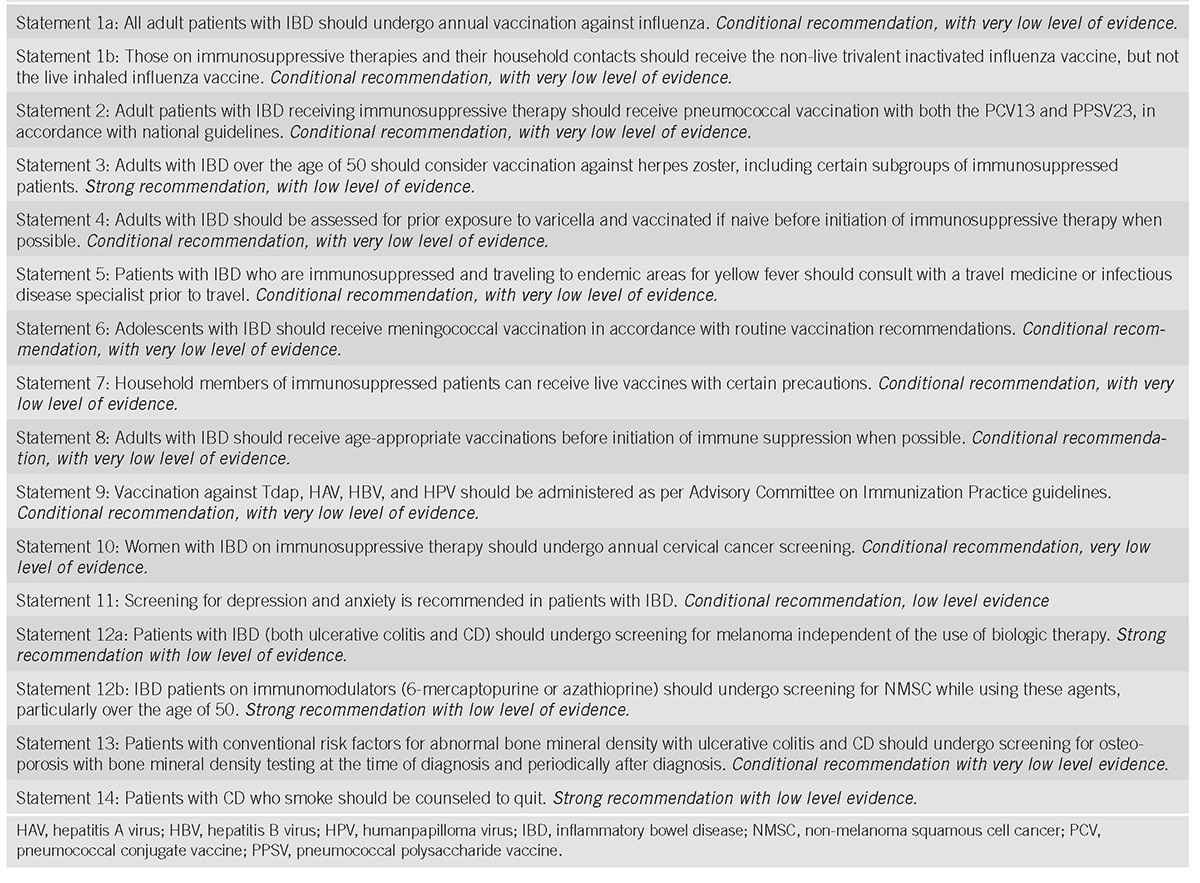
To evaluate the level of evidence and strength of recommendations, we used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system (1). The level of evidence could range from “high” (implying that further research was unlikely to change the authors’ confidence in the estimate of the effect), “moderate” (further research would be likely to have an impact on the confidence in the estimate of effect), “low” (further research would be expected to have an important impact on the confidence in the estimate of the effect and would be likely to change the estimate), or “very low” (any estimate of effect is very uncertain). The strength of a recommendation was graded as “strong” when the desirable effects of an intervention clearly outweigh the undesirable effects and as “conditional” when there is uncertainty about the trade-offs. We preferentially used meta-analyses or systematic reviews when available, followed by clinical trials and retrospective cohort studies. To determine the level of evidence, we entered data for the papers of highest evidence into the GRADE program (accessible at http://www.gradepro.org). The GRADE recommendations statements from this guideline are in Table 1. Summary statements are descriptive and do not have associated evidence-based ratings (Table 2). In this guideline, the numbered statements are the GRADE statements and the unnumbered statements relate to summary statements.

Summary and strength of recommendationsContinuedContinued

Continued

Continued

Summary statementsContinuedContinued

Continued

Continued
CLINICAL FEATURES
Hallmark/cardinal symptoms of Crohn’s disease include abdominal pain, diarrhea, and fatigue; weight loss, fever, growth failure, anemia, recurrent fistulas, or extraintestinal manifestations can also be presenting features (Summary Statement).
The most common symptom of Crohn’s disease is chronic diarrhea, but some patients may not experience this symptom (2). Abdominal pain, often localized to the right lower quadrant of the abdomen and worsened postprandially, is common. Fatigue is also a very prevalent symptom in Crohn’s disease and is thought to arise from a number of factors including inflammation itself, anemia, or various vitamin and mineral deficiencies. Some patients will present with constitutional signs or symptoms including fever, weight loss or, in the case of younger patients, growth failure.
Crohn’s disease is diagnosed clinically. There are no truly pathognomonic features. Endoscopic, radiographic, and histologic criteria with evidence of chronic intestinal inflammation will be present (Summary Statement).
The clinician must integrate multiple streams of information, including history and physical, laboratory tests, endoscopy results, pathology findings, and radiographic tests, to arrive at a clinical diagnosis of Crohn’s disease. In general, it is the presence of chronic intestinal inflammation that solidifies a diagnosis of Crohn’s disease. Distinguishing Crohn’s disease from ulcerative colitis can be challenging when inflammation is confined to the colon, but clues to the diagnosis include discontinuous involvement with skip areas, sparing of the rectum, deep/linear/serpiginous ulcers of the colon, strictures, fistulas, or granulomatous inflammation. Granulomas are present on biopsy in only a minority of patients. The presence of ileitis in a patient with extensive colitis (“backwash ileitis”) can also make determination of the IBD subtype challenging.
Extraintestinal manifestations of Crohn’s disease include the classic ones such as arthropathy (both axial and peripheral); dermatological (including pyoderma gangrenosum and erythema nodosum); ocular (including uveitis, scleritis, and episcleritis); and hepatobiliary disease (i.e., primary sclerosing cholangitis). Other extraintestinal complications of Crohn’s disease include: thromboembolic (both venous and arterial); metabolic bone diseases; osteonecrosis; cholelithiasis; and nephrolithiasis. A number of other immune-mediated diseases are associated with Crohn’s disease, including asthma, chronic bronchitis, pericarditis, psoriasis, celiac disease, rheumatoid arthritis, and multiple sclerosis (Summary Statement).
A systematic review of population-based cohort studies of adult patients with Crohn’s disease identified an increased risk of bone fractures (30–40% elevation in risk), and thromboembolism (3-fold higher risk) (3). A variety of extraintestinal manifestations, including primary sclerosing cholangitis, ankylosing spondylitis, uveitis, pyoderma gangrenosum, and erythema nodosum, have been observed in patients with Crohn’s disease. Moreover, there are weak associations between Crohn’s disease and other immune-mediated conditions, such as asthma, psoriasis, rheumatoid arthritis, and multiple sclerosis.
NATURAL HISTORY
Crohn’s disease, in most cases, is a chronic, progressive, destructive disease (Summary Statement).
The chronic intestinal inflammation that occurs in Crohn’s disease can lead to the development over time of intestinal complications such as strictures, fistulas, and abscesses. These complications can lead to inhibition of intestinal function or to surgery that itself can result in some morbidity and loss of intestinal function. A scoring system, the Lémann index, has been created to quantify the degree of bowel damage incurred by intestinal complications and subsequent surgery (4). This index has been shown to be reproducible and internally consistent, and median index scores rise with disease duration (5). In a population-based cohort study from Olmsted County, Minnesota, of 147 Crohn’s disease patients who had undergone at least 1 bowel resection (median follow-up per patient, 13.6 years), the median cumulative length of bowel resected was 64 cm, and the median rate of bowel resection was 4.2 cm annually (6).
The location of Crohn’s disease tends to be stable, but can occasionally extend (Summary Statement).
Population-based studies from Norway and Minnesota suggest that Crohn’s disease presents with ileal, ileocolonic, or colonic disease in roughly one-third of patients each, and that only a small minority of patients (6–14%) will have a change in disease location over time (7,8,9).
Most, but not all, patients with Crohn’s disease will present with non-penetrating, non-stricturing disease behavior, but up to half of patients would have developed an intestinal complication (i.e., stricture, abscess, fistula, or phlegmon) within 20 years of diagnosis. Patients with ileal, ileocolonic, or proximal gastrointestinal (GI) involvement are significantly more likely than those with isolated colonic disease to progress to an intestinal complication. Extensive anatomic involvement and deep ulcerations are other risk factors for progression to intestinal complications (Summary Statement).
Multiple population-based cohorts of Crohn’s disease have demonstrated that the majority of patients (between 56% and 81%) have inflammatory disease behavior at diagnosis, whereas between 5% and 25% each present with stricturing or penetrating disease behavior (9). A population-based study from Olmsted County showed that the cumulative risk of developing an intestinal complication among those presenting with inflammatory behavior was 51% at 20 years after diagnosis.(10). Multivariate analysis demonstrated that ileal, ileocolonic, or upper GI involvement, relative to colonic involvement, were significantly associated with faster time to the development of intestinal complications.
Over long periods of observation, only 20–30% of patients with Crohn’s disease will have a nonprogressive or indolent course. Therefore, the majority of patients will require active effort to identify therapies that achieve adequate control of bowel inflammation (Summary Statement).
Features that are associated with a high risk for progressive disease burden include young age at diagnosis (11), initial extensive bowel involvement, ileal/ileocolonic involvement, perianal/severe rectal disease, and patients presenting with a penetrating or stenosis disease phenotype (12). Visceral adiposity may be a marker for increased risk of penetrating disease (13) (Summary Statement).
Symptoms of Crohn’s disease do not correlate well with the presence of active inflammation, and therefore should not be the sole guide for therapy. Objective evaluation by endoscopic or cross-sectional imaging should be undertaken periodically to avoid errors of under- or overtreatment (Summary Statement).
Perianal fistulizing Crohn’s disease occurs in up to one-quarter of patients (Summary Statement).
In population-based cohorts, the frequency of perianal fistulas is between 10 and 26%, and the cumulative risk was 26% at 20 years after diagnosis in one cohort (9,14,15). Perianal disease at diagnosis may indicate a more severe clinical course of Crohn’s disease.
Symptoms of Crohn’s disease occur in most cases as a chronic, intermittent course; only a minority of patients will have continuously active symptomatic disease or prolonged symptomatic remission (Summary Statement).
A population-based study from Olmsted County, Minnesota, modeled the lifetime course of Crohn’s disease in various disease states using a Markov model; the model was unique in that the transition probabilities between disease states were derived by mapping disease states to the actual chronological history of each patient (16). Over the lifetime disease course, a representative patient spent 24% of the duration of their disease in a state of medical remission, 27% in mild disease, 1% in severe drug-responsive disease, 4% in severe drug-dependent disease, 2% in severe drug-refractory disease, 1% in surgery, and 41% in postsurgical remission. In the 1962–1987 Copenhagen County cohort, within the first year after diagnosis, the proportions of patients with high activity, low activity, and clinical remission were 80%, 15%, and 5%, respectively (17). However, after the first year through 25 years, a decreasing proportion of high activity (30%), increasing proportion of remission (55%), and stable proportion of mild activity (15%) were observed.
In the absence of immunomodulator or biologic treatment, steroid dependency and/or resistance occurs in up to half of patients (Summary Statement).
Population-based studies from Denmark and Minnesota suggest that between 43 and 56% of Crohn’s disease patients received corticosteroids in the prebiologic era, and that over half of these patients were either steroid dependent, steroid refractory, or required surgical resection within the subsequent year (18,19).
Up to 80% of patients with Crohn’s disease require hospitalization at some point during their clinical course, but the annual hospitalization rate decreases in later years after diagnosis (Summary Statement).
An older Copenhagen County study suggested that 83% of patients were hospitalized within 1 year of diagnosis, and the annual rate of hospitalization thereafter was about 20% (18). Up to 70% of Olmsted County patients were hospitalized at least once, and the cumulative risk of hospitalization in the prebiologic era was 62% at 10 years. The annual rate of hospitalization was highest in the first year after diagnosis (15).
The 10-year cumulative risk of major abdominal surgery in Crohn’s disease is 40% to 55%, although recent studies performed in the biologic era suggest that the 10-year risk may have decreased to 30%. The 10-year risk of a second resection after the first is 35%, although again more recent studies suggest that this may have dropped to closer to 30% (Summary Statement).
In a systematic review of 30 publications examining major abdominal surgical risk in Crohn’s disease, the cumulative incidence of surgery was 46.6% at 10 years, and that this risk was reported to be lower, under 40%, among patients who had been diagnosed after 1980 (20). Another systematic review examined the risk of a second resection among those Crohn’s disease patients who had undergone a first resection, and this was estimated to be 35% at 10 years overall, but significantly lower among those patients diagnosed after 1980 (21).
In Crohn’s disease, the 5-year rate of symptomatic post-operative recurrence is ∼50% (Summary Statement).
Among Crohn’s disease patients who undergo major abdominal surgery, the 5-year cumulative risk of clinical recurrence is 40% to 50% (22,23). The risk of endoscopic recurrence approaches 90%. Risk factors for recurrent Crohn’s disease postoperatively include cigarette smoking, shorter duration of disease before operation, more than one resection, and penetrating complications.
Overall mortality in Crohn’s disease is slightly increased, with a standardized mortality ratio of 1.4 times that of the general population. Causes of excess mortality include GI disease, GI cancer, lung disease, and lung cancer (Summary Statement).
A 2007 meta-analysis of 13 studies of Crohn’s disease mortality yielded a pooled standardized mortality ratio of 1.5 (24). There was a nonsignificant trend for decreased mortality in more recent studies. In a 2013 meta-analysis, the pooled standardized mortality ratio for Crohn’s disease was 1.46, and slightly lower at 1.38 when restricted to population-based and inception studies (25). Several studies have demonstrated an association between current use of corticosteroids and increased mortality in Crohn’s disease (26,27).
INTESTINAL MALIGNANCY
Patients with colonic involvement are at increased risk of colorectal cancer, and risk factors include duration of disease, extent of colonic involvement, primary sclerosing cholangitis, family history of colorectal cancer, and severity of ongoing colonic inflammation (Summary Statement).
Crohn’s disease patients with colitis are at increased risk of colorectal cancer (28). Similar to ulcerative colitis, risk factors for colorectal cancer include duration of Crohn’s, primary sclerosing cholangitis, and family history of colorectal cancer.
Patients with small bowel involvement are at increased risk of small bowel adenocarcinoma that can be difficult to diagnose preoperatively (Summary Statement).
The relative risk of small bowel adenocarcinoma in patients with Crohn’s disease is markedly elevated (at least 18-fold), although the absolute risk remains low, in the order of 0.3 cases per 1,000 patient-years (29). The increased risk is thought to arise from longstanding chronic inflammation.
DIAGNOSIS
The diagnosis of Crohn’s disease (CD) is based on a combination of clinical presentation and endoscopic, radiologic, histologic, and pathologic findings that demonstrate some degree of focal, asymmetric, and transmural granulomatous inflammation of the luminal GI tract (30,31). Laboratory testing is complementary in assessing disease severity and complications of disease. There is no single laboratory test that can make an unequivocal diagnosis of CD. The sequence of testing is dependent on presenting clinical features.
Routine laboratory investigation
Initial laboratory investigation should include evaluation for inflammation, anemia, dehydration, and malnutrition (Summary Statement).
In patients who have symptoms of active Crohn’s disease, stool testing should be performed to include fecal pathogens, Clostridium difficile testing, and may include studies that identify gut inflammation such as a fecal calprotectin (Summary Statement).
Recommendations.
- Fecal calprotectin is a helpful test that should be considered to help differentiate the presence of IBD from irritable bowel syndrome (strong recommendation, moderate level of evidence).
Patients presenting with suspected CD often will show laboratory evidence of inflammatory activity. Anemia and an elevated platelet count are the most common changes seen in the complete blood count (32,33). Serum C-reactive protein (CRP) is an acute-phase reactant produced by the liver that goes up with inflammation seen in a subset of patients with CD. It has a short half-life of 19 hours. Because of its short half-life, serum concentrations decrease quickly, making CRP a useful marker to detect and monitor inflammation (see later section) (34,35). Erythrocyte sedimentation rate is also a nonspecific measure of inflammation that may be elevated in patients with Crohn’s disease. Erythrocyte sedimentation rate may be useful in an individual patient but does not discriminate IBD patients from those with irritable bowel syndrome or healthy controls (36). Up to 40% of IBD patients with mild inflammation may have a normal CRP and erythrocyte sedimentation rate that may limit the usefulness of these markers in monitoring some patients (37). Signs and symptoms of bowel inflammation related to IBD overlap with infectious enteritis and colitis. Stool studies for fecal pathogens and C. difficile will help direct diagnosis and management. Fecal calprotectin is a calcium binding protein that is derived from neutrophils and plays a role in the regulation of inflammation. Fecal lactoferrin is an iron binding protein found in secondary granules of neutrophils. These serve as noninvasive markers of intestinal inflammation. They are useful in differentiating patients with IBD from those with irritable bowel syndrome (38,39,40,41,42). Fecal markers may also be useful in monitoring disease activity and response to treatment (see later section).
Genetic testing
Genetic testing is not indicated to establish the diagnosis of Crohn’s disease (Summary Statement).
Certain genetic variants are associated with different phenotypic expressions in Crohn’s disease but testing remains a research tool at this time (Summary Statement).
CD is a heterogeneous disease with complex interactions between genetics, environmental exposures, and the intestinal microbiome. To date, there are over 200 genetic loci associated with IBD and greater than 71 CD susceptibility loci that have been identified through large-scale genome-wide association studies (43,44,45). As more genetically diverse populations are studied, this is likely to expand. Examples of single-nucleotide polymorphisms that confer susceptibility to CD include sequences in the NOD2 gene, the interleukin (IL)-23 receptor gene, and the autophagy-related 16-like 1 (ATG16L1) gene (46). These genes play a role in innate immunity and regulation of the epithelial barrier (47). These susceptibility variants are biologically important in understanding the pathophysiology of CD, but there is no single variant that has a high enough frequency in the CD population to make it diagnostically useful. There is significant variation in the prevalence of susceptibility genes between various racial/ethnic groups—for example, NOD2 and IL23R variants are very uncommon in East Asian populations (43). There are genetic variants that are associated with disease phenotype. NOD2 variants are predictors of a more complicated disease behavior including ileal involvement, stenosis, and penetrating disease behaviors and the need for surgery (48). These variants are also associated with early disease onset (49). IL-12B variants are associated with the need for early surgery (50). NOD2 testing is commercially available for three of the most common variants seen in CD. Although identification of these variants may identify patients who are likely to have more aggressive CD, this laboratory test has not been routinely used clinically and remains a research tool. Ultimately, we may be able to use genetic testing to characterize patient’s disease behavior and guide early therapy (51).
Serologic markers of IBD
Routine use of serologic markers of IBD to establish the diagnosis of Crohn’s disease is not indicated (Summary Statement).
Because of the heterogeneous nature of IBD there has been extensive research directed toward finding immunologic markers that would assist in disease diagnosis. These studies have focused on antibodies to microbial antigens and autoantibodies (Supplementary Information online). Anti-glycan antibodies are more prevalent in CD than in ulcerative colitis but have a low sensitivity, making their use in diagnosis less helpful (52).
Endoscopy
Ileocolonoscopy with biopsies should be performed in the assessment of patients with suspected Crohn’s disease (Summary Statement).
Disease distribution and severity should be documented at the time of diagnosis. Biopsies of uninvolved mucosa are recommended to identify extent of histologic disease (Summary Statement).
Colonoscopy with intubation of the terminal ileum and biopsy is recommended as part of the initial evaluation of patients with suspected IBD. Over 80% of patients with IBD will have mucosal involvement within the reach of the colonoscope. Ileal intubation rates via colonoscopy are as high as 80–97% in patients in whom the cecum is reached (53). Small bowel follow-through barium examinations of the terminal ileum may both over- and under-represent disease of the ileum (53,54). Direct evaluation of the ileum will complement radiographic findings in the diagnosis of CD. Mucosal changes suggestive of CD include mucosal nodularity, edema, ulcerations, friability, and stenosis (53,55). Classical granulomatous inflammation is seen in a minority of patients (up to 33%) with CD, and is helpful, but not required, for diagnosis. Disease distribution of endoscopic and histologic findings is important to document at the time of diagnosis, as this has implications on screening for colorectal cancer, disease prognosis, and ultimately affect therapeutic decision making. Attempts to quantify the distribution and severity of mucosal involvement of the colon and the ileum in patients with CD have led to the development of multiple endoscopic scoring systems, including the Crohn’s Disease Endoscopic Index of Severity (CDEIS) and the Simple Endoscopic Score for Crohn’s disease (SES-CD) (56,57). The SES-CD is the least cumbersome to use and has been incorporated into many commercial endoscopic reporting systems (57) (Supplementary Information online). Studies using central endoscopy readers have shown excellent intra- and inter-rater reliability (58) (see later section).
Upper endoscopy should only be performed in patients with upper GI signs and symptoms (Summary Statement).
The presence of CD of the upper GI tract is often underestimated, with most studies in adults suggesting that the prevalence range is 0.3–5% (59). Looking at the incidence prospectively, this number is higher, in the range of 16% of patients showing endoscopic and histologic changes consistent with CD. Of this group of patients, only ∼37% were symptomatic at the time of evaluation (60). Routine endoscopic evaluation in asymptomatic CD patients is associated with mild endoscopically visible inflammation in up to 64% of patients and histologic inflammation in up to 70% of patients (61). These studies have been carried out predominately in children. Despite these findings there does not appear to be any clinical significance related to these mild changes (62). Endoscopic features suggestive of CD include mucosal nodularity, ulceration (both aphthous and linear), antral thickening, and duodenal strictures (63). Histologic changes may include granulomatous inflammation, focal cryptitis of the duodenum, and focally enhanced gastritis (60).
Video capsule endoscopy is a useful adjunct in the diagnosis of patients with small bowel Crohn’s disease in patients in whom there is a high index of suspicion of disease (Summary Statement).
Patients with obstructive symptoms should have small bowel imaging and/or patency capsule evaluation before video capsule endoscopy to decrease risk of capsule retention (Summary Statement).
Small bowel capsule endoscopy allows for direct visualization of the mucosa of the small intestine. Isolated small bowel involvement may be seen in up to 30% of patients with CD, making it more challenging to diagnose with routine small bowel imaging techniques (64). Several meta-analyses have examined the diagnostic yield of capsule endoscopy in the evaluation of patients with suspected CD. Capsule endoscopy is superior to small bowel barium studies, computed tomography enterography (CTE) and ileocolonoscopy in patients with suspected CD, with incremental yield of diagnosis of 32%, 47%, and 22% respectively (64). However, some studies have questioned the specificity of capsule endoscopy findings for CD, and to date there is no consensus as to exactly which capsule endoscopy findings constitute a diagnosis of CD (65). The Lewis score is a scoring system based on the evaluation of three endoscopic parameters: villous appearance, ulcers, and strictures. The scoring system is incorporated into the software platform of the some endoscopy capsules and assists in the quantification of small bowel inflammatory burden and diagnosis of CD (66). Capsule endoscopy has a high negative predictive value of 96% (67). The capsule retention rate in patients with suspected CD is 0–5.4%, and higher in those with known CD (68). Use of a patency capsule or small bowel imaging before video capsule endoscopy will reduce the risk of retention of the standard video capsule (69,70,71). Capsule endoscopy may identify a site for directed biopsy to obtain tissue to establish a diagnosis of CD.
Deep enteroscopy is not part of routine diagnostic testing in patients with suspected Crohn’s disease, but may provide additional information in patients who require biopsy/sampling of small bowel tissue to make a diagnosis (Summary Statement).
Capsule endoscopy and small bowel imaging techniques lack the means to provide tissue when that is needed for diagnosis during evaluation of the small bowel. Device-assisted enteroscopic techniques, which include single-balloon enteroscopy (Olympus, Tokyo, Japan) and double-balloon enteroscopy (Fujinon, Tokyo, Japan and NaviAid, Pentax), have been developed to allow for deep enteroscopic evaluation of the small bowel (72). Double-balloon enteroscopy studies in CD have not included large numbers of patients, but report a diagnostic yield as high as 80% when used in patients with suspected CD (73,74,75,76). Double-balloon enteroscopy is more sensitive in detecting lesions in patients with suspected CD than multiple radiographic imaging techniques (77); however, because of the invasive and potentially time-consuming nature of the study, it should be reserved for cases in which tissue is needed or potential therapeutic intervention such as stricture dilation is required (72).
Recommendations.
- In patients at particularly high risk for colorectal neoplasia (e.g., personal history of dysplasia, primary sclerosing cholangitis), chromoendoscopy should be used during colonoscopy, as it may increase the diagnostic yield for detection of colorectal dysplasia, especially compared with standard-definition white light endoscopy (conditional recommendation, low level of evidence).
- For patients undergoing surveillance colonoscopy there is insufficient evidence to recommend universal chromoendoscopy for IBD colorectal neoplasia surveillance, if the endoscopist has access to high-definition white light endoscopy (conditional recommendation, moderate level of evidence).
Surveillance colonoscopy is suggested for patients who have a minimum of 8 years of disease who have 30% or more of their colon involved. The risk of neoplasia in Crohn’s colitis increases with both the duration and the extent of disease. Those individuals with primary sclerosing cholangitis should initiate surveillance colonoscopy at the time of their diagnosis regardless of disease distribution. We currently do not recommend routine surveillance for small bowel Crohn’s disease. Chromoendoscopy should be done in the setting of endoscopic remission. There have been suggested methods to perform chromoendoscopy (78). A 2011 meta-analysis of 6 studies involving over 1,200 IBD patients saw a 7% incremental improvement in dysplasia detection yield over standard-definition white light colonoscopy (79). In a randomized controlled trial comparing white light high-definition endoscopy with dye spraying chromoendoscopy and electronic virtual colonoscopy in 270 IBD patients with longstanding ulcerative colitis or Crohn’s colitis, there was no significant difference in dysplasia detection rates between the three modalities—high-definition white light colonoscopy alone was sufficient for detecting colorectal neoplasia (80). Another randomized controlled trial (involving a total of 103 patients) comparing high-definition white light endoscopy with chromoendoscopy in ulcerative colitis has been presented in a preliminary manner (81). In this case, the dysplasia detection rate was significantly higher among the 50 patients randomized to chromoendoscopy (22%) compared with that of the 53 patients randomized to high-definition white light endoscopy (9.4%) (81). A 2017 systematic review evaluated 10 randomized trials that included 1,500 patients to compare chromoendoscopy with other endoscopic techniques for dysplasia surveillance in patients with IBD (82). Chromoendoscopy was significantly associated with a higher likelihood of detecting patients with dysplasia compared with other techniques (relative risk (RR), 1.37; 95% confidence interval (CI), 1.04–1.79); this association was significant only if chromoendoscopy was compared with standard-definition white-light endoscopy (RR, 2.12; 95% CI, 1.15–3.91). When chromoendoscopy was compared with high-definition white light endoscopy it was not more likely to detect dysplasia (RR, 1.42; 95% CI, 0.80–2.52). Chromoendoscopy required a significantly longer procedural time compared with other techniques (mean difference, 8.91 min; 95% CI, 1.37–16.45) (83). There was no direct evidence of effect on preventing all-cause/cancer-specific mortality or time to interval cancer. At this point in time, there is not sufficient evidence to strongly recommend universal chromoendoscopy for IBD colorectal neoplasia surveillance if the endoscopist has access to high-definition white light endoscopy.
Recommendations.
- Narrow-band imaging should not be used during colorectal neoplasia surveillance examinations for Crohn’s disease (conditional recommendation, very low level of evidence).
There was hope that narrow-band imaging would serve as a virtual chromoendoscopy and increase dysplasia detection over white light endoscopy without the need for actual dye spraying. A randomized trial from Barcelona of 60 patients with longstanding colonic IBD compared narrow-band imaging with dye spraying chromoendoscopy, and there was no difference in dysplasia detection rates (84). Another randomized trial comparing narrow-band imaging with high-definition white light endoscopy for neoplasia surveillance in patients with longstanding ulcerative colitis could not detect a difference in dysplasia detection rates (85). Thus, narrow-band imaging cannot be recommended as a surveillance tool in patients with longstanding colitis.
Recommendations.
- Endoscopists who are sufficiently trained and comfortable performing chromoendoscopy may be able to forgo obtaining random surveillance biopsies and rely on targeted biopsies alone (conditional recommendation, very low level of evidence).
Multiple studies have found that the rate of dysplasia detection from random, nontargeted biopsies is extremely low, in the order of 0.1 to 0.2%, whereas the detection rate in targeted biopsies is considerably higher—indeed, in such comparison studies, the percentage of dysplastic lesions detected on targeted biopsies ranges from 80 to 90% (86,87,88,89,90). Thus, endoscopists sufficiently trained in chromoendoscopy can rely on targeted biopsies alone. The learning curve for performing chromoendoscopy may not be steep—in one recent study, there was no difference in dysplasia detection rates between expert and nonexpert endoscopists (18.5% vs. 13.1%) (91).
Imaging studies
Small bowel imaging should be performed as part of the initial diagnostic workup for patients with suspected Crohn’s disease (Summary Statement).
Computed tomography enterography (CTE) is sensitive for the detection of small bowel disease in patients with Crohn’s disease and is comparable to magnetic resonance enterography (MRE) (Summary Statement).
Because of the absence of any radiation exposure, MRE should be used preferentially in young patients (<35 years) and in patients in whom it is likely that serial exams will need to be performed (Summary Statement).
The decision for which small bowel imaging study to use is in part related to the expertise of the institution and the clinical presentation of the patient (Summary Statement).
The small bowel is one of the most common areas affected by inflammation in patients with CD. Much of the inflammation is beyond the reach of standard endoscopic evaluation. In up to 50% of patients with active small bowel disease, inflammation may skip the terminal ileum or be intramural and not detected by ileocolonoscopy (92). Complications of CD such as stricturing disease and enteric fistulas are best identified using small bowel imaging techniques. CTE has a reported sensitivity as high as 90% in detecting lesions associated with CD (65,93). The sensitivity for detecting active small bowel CD in one comparison study was only 65% with small bowel follow-through compared with 83% with CTE (65). In studies comparing capsule endoscopy with small-bowel follow-through, there have been instances of patients with a normal small bowel follow-through showing both mucosal disease (20%) and stricturing disease (6%) on a capsule endoscopy (94). CTE features such as mucosal enhancement, mesenteric hypervascularity, and mesenteric fat stranding are all suggestive of active inflammation (95). MRE has similar sensitivity to CTE with wall enhancement, mucosal lesions, and T2 hypersensitivity as suggestive of intestinal inflammation (96). Inflammation scoring systems have been developed to provide quantification of the degree of inflammation. This may allow for assessment of treatment effects in serial examinations (97). Improvement in radiologic parameters for CTE and MRE with medical therapy is associated with a better clinical outcome in terms of hospitalization, surgery, and steroid use in patients with small bowel CD (98). In patients with CD the need for sequential imaging exams is seen in young patients, patients with upper GI disease, patients with penetrating disease, and patients who require steroids, biologics, and surgery. The need for repeated CTE studies over time leads to levels of diagnostic radiation exposure that theoretically might significantly increase cancer risk (99,100). In these patients MRE is preferred. Techniques to reduce dose of radiation exposure during diagnostic CT scanning have been implemented and currently being refined using changes in both software and hardware to maintain image quality with a decreased dose of radiation. How this will alter the use of CTE is not known (101).
Cross-sectional imaging with MRI of the pelvis and/or endoscopic ultrasound may be used to further characterize perianal Crohn’s disease and perirectal abscesses (Summary Statement).
Approximately 25% of patients with CD will develop a perirectal complication of their disease, including fistula formation and/or perirectal abscess (14). With standard medical therapy there is a high relapse rate of fistulous drainage. Imaging of the perianal area allows for identification of disease that requires surgical intervention to help with healing as well identify and classify all of the disease that is present before and after medical therapy (102). Comparison studies have shown endoscopic ultrasound to have greater than 90% accuracy in diagnosis of perianal fistulizing disease.(103) Serial endoscopic ultrasound exams may be used to help guide therapeutic intervention in patients with perianal Crohn’s fistulizing disease, including seton removal and discontinuation of medical therapy (104,105). Magnetic resonance imaging (MRI) of the pelvis has comparable accuracy (102,106).
If an intra-abdominal abscess is suspected, cross-sectional imaging of the abdomen and pelvis should be performed (Summary Statement).
CTE and MRE both have an accuracy of >90% in the detection of abscesses preoperatively (107). CT can be used to help direct abscess drainage preoperatively that may lead to a lower rate of postsurgical complications (108).
Determining disease activity and distribution
IBD type, location, and disease activity should be documented in the medical record (Summary Statement).
The disease course of CD and decisions focusing on appropriate immediate and future therapy are in part predicted by clinical features at the time of diagnosis. These features include age of onset, disease distribution, disease activity, and disease phenotype. Documentation of these features in the medical record is part of multiple quality initiatives in the care of patients with IBD, although it is not included as part of the 2015 changes in the Physician Quality Reporting System quality reporting requirements (109,110). Documentation of disease activity at each encounter lends itself to the monitoring of disease progression and efficacy of therapy (111).
Disease activity.
Clinical disease activity in CD is divided into remission, mild, moderate, and severe. There is no “gold standard” for determining disease activity. Disease activity depends on heterogeneous clinical measures, impact on quality of life, complications of disease, and complications of therapy. Despite the difficulty in the assessment of clinical activity, these assessments are important in that they allow the clinician to make decisions about disease management. Mild disease is characterized by patients who are ambulatory and are eating and drinking normally (112). There is <10% weight loss and there are no complications such as obstruction, fever, abdominal mass, or dehydration. These patients may have diarrhea and abdominal pain and the serum CRP is usually increased. With mild disease there is minimal impact on quality-of-life indices. This correlates to a Crohn’s Disease Activity Index (CDAI) score of 150–220. Those patients with severe disease may be cachectic with significant weight loss. They may have complications such as obstruction or intra-abdominal abscess. Symptoms persist despite aggressive therapy. These patients are often hospitalized. This corresponds to a CDAI of >450. Those with moderate disease fit in between the extremes. Of note, symptomatic disease activity is not directly correlated with natural history.
Indices that are commonly used in clinical trials include the CDAI, the Harvey Bradshaw Index and patient-reported outcome tools (see Supplementary Information online). This will be further discussed in the section “Working Definitions of Disease Activity and Prognosis.”
Phenotypic classification.
The international standard of phenotypic classification is currently the 2005 Montreal revision of the Vienna classification (113). This classification system includes age of onset, disease location, and disease behavior. A1 refers to disease onset at 16 years of age or younger, A2 disease onset between 17 and 40 years of age, and A3 over 40 years. Disease location is divided into L1 (terminal ileum), L2 (colon), L3 (ileocolonic), and L4 (upper GI involvement). Disease behavior is divided into B1 (nonstricturing, nonpenetrating), B2 (structuring), and B3 (penetrating). The letter “p” is appended to the B subtype if there is the presence of perianal fistulizing disease (114). Location tends to remain stable and behavior tends to progress from B1 to B2 or B3 over the course of disease. The Paris classification further divides age into smaller segments and breaks down upper GI disease to location above and below the ligament of Treitz (115). These subclassifications appear to be most useful in the pediatric population.
Monitoring disease activity
The goals of therapy in IBD have historically been based on symptomatic response with good control of symptoms and improved quality of life. We now have objective measures of inflammation that may allow tighter control of the inflammatory process. Monitoring of the inflammatory response includes fecal markers, serum markers, imaging studies, and endoscopic assessment. The concept of “treating to target” is using the assessment of response of both clinical and inflammatory parameters to define remission. What is not clear is whether this rigorous definition of remission will lead to long-term improvement of outcomes or modify the disease course. With the advances that have been made in the medical therapy of CD, the concept of treating to target is becoming more realistic but there is still a need to have long-term observational studies to see whether complete clinical and inflammatory remission is required in all patients (116,117,118).
Fecal calprotectin and fecal lactoferrin measurements may have an adjunctive role in monitoring disease activity (Summary Statement).
Fecal markers may have a role in noninvasively monitoring disease activity in CD. Studies have shown that both fecal lactoferrin and fecal calprotectin are sensitive markers of disease activity and correlate with a number of the endoscopic activity indices such as the colonic SES-CD (119,120). There have been several studies that suggest that levels of fecal calprotectin can be used to monitor patients for postoperative recurrence after ileocolic resection for Crohn’s disease. Levels of >100 μg/g indicate endoscopic recurrence with a sensitivity in the range of 89% (121,122). In patients with an infliximab-induced remission, fecal calprotectin of >160 μg/g has a sensitivity of 91.7% and a specificity of 82.9% to predict relapse (123,124).
Serum CRP is relatively nonspecific for the inflammation of Crohn’s disease, but in select patients serial measurements may have a role in monitoring disease activity and response to therapy (Summary Statement).
Serum CRP has been shown to have a more consistent role in monitoring response in patients treated with infliximab. High levels at baseline (>15 mg/l) predict primary nonresponse to infliximab with 67% sensitivity and 65% specificity (125). Normalization of CRP during infliximab therapy at 14 weeks is associated with a greater chance of continued response or remission during maintenance therapy (126).
Periodic cross-sectional imaging (CTE, MRE) may be considered in monitoring response to therapy in certain patients with small bowel Crohn’s disease (Summary Statement).
MR inflammatory scores have been developed that may allow for serial MRI to determine response to therapy (127,128). Improvement in MR inflammatory scores correlates with clinical improvement in patients treated with infliximab (129). It has also been demonstrated that an improvement in MRE and CTE inflammatory parameters is associated with a decrease in hospitalizations, surgery, and steroid requirements in patients with small bowel CD (98). The ability to examine the entire bowel wall for changes associated with inflammation is advantageous in populations of patients who cannot be assessed endoscopically (e.g., patients with primarily small intestinal involvement). Small bowel ultrasound has been used largely outside the United States for evaluation of CD. It has been used to assist in the diagnosis of CD, for detection of extramural complications, for the detection and evaluation of stenotic strictures, and for follow-up of the disease course.
Mucosal healing as determined by endoscopy is a goal of therapy (Summary Statement).
- Endoscopic scores have been developed that are reliable in measuring degree of mucosal healing and may be used to monitor response to therapy.
- Evaluation of the ileum for postoperative endoscopic recurrence by colonoscopy within a year after ileocolonic resection may help guide further therapy.
Mucosal healing has become an important target in assessing efficacy of treatment for IBD. In patients with CD, mucosal healing is defined as an absence of ulceration and endoscopic scoring systems have been developed to quantify degree of ulceration and inflammation in patients with CD within the reach of the colonoscope (130). There are a limited number of studies that have examined the long-term impact of mucosal healing on the clinical course of disease. In patients with early-stage CD, complete mucosal healing after 2 years of therapy predicts sustained steroid-free, clinical remission 3 and 4 years out from initiation of treatment (131). Other clinical outcomes associated with mucosal healing in CD have been decreased surgery and hospitalizations (132). The SES-CD (57) scoring system has been used prospectively to assess mucosal healing in patients treated with anti-tumor necrosis factor (anti-TNF) therapy as well as with anti-TNF/thiopurines combination therapy, demonstrating that changes can be measured; furthermore, there is a strong correlation between improvement in the SES-CD (mucosal) healing and clinical remission (133,134). In the patient who has undergone an ileocolonic resection, assessment of endoscopic lesions just proximal to the anastomosis appears to identify patients who are likely to have a clinical recurrence of CD (135). This endoscopic activity score is known as the Rutgeerts’ score and has become widely used in the assessment of postoperative patients (136) (Supplementary Information online).
Disease modifiers
Recommendations.
- Nonsteroidal anti-inflammatory drugs (NSAIDs) may exacerbate disease activity and should be avoided when possible in patients with Crohn’s disease (strong recommendation, low level of evidence).
There are numerous case reports and observational studies that suggest that use of NSAIDs in patients with CD are associated with IBD flares. NSAIDs have been documented to damage the mucosa of the small intestine distal to the duodenum with ulcerations, erosions, and webs. Mucosal permeability is increased with NSAID therapy leading to increased exposure to luminal toxins and antigens (137). In a comparison study of acetaminophen, naproxen, nabumetone, nimesulide, and aspirin, there was a 17–28% relapse rate of quiescent IBD within 9 days of therapy with the nonselective NSAIDS (naproxen and nabumetone) (138). Recent NSAID use has been associated with an increased risk of emergency admission to the hospital for patients with IBD (139,140). There have been other studies that have not found this association (141). Selective cyclooxygenase-2 inhibitors in short-term therapy have not been shown to exacerbate ulcerative colitis, but similar studies have not been performed in CD (142).
Recommendations.
- Cigarette smoking exacerbates disease activity and accelerates disease recurrence and should be avoided. Active smoking cessation programs should be encouraged (strong recommendation, low level of evidence).
Cigarette smoking has been shown in multiple clinical situations to have an adverse effect on disease activity in CD. There is an increased rate of surgical intervention, incidence of IBD hospitalizations, and peripheral arthritis in patients with CD who smoke as compared with those who do not smoke (143,144). Active smoking has been associated with a penetrating phenotype in CD (145). Active smoking increases the risk of relapse after discontinuation of anti-TNF therapy (146). Patients with CD who stop smoking have decreased flares in disease activity and a decreased need for steroids and immunomodulatory therapy (147).
Recommendations.
- Usage of antibiotics should not be restricted in Crohn’s disease patients in order to prevent disease flares (Conditional recommendation, very low level of evidence).
The intestinal microbiome is thought to play a role in the pathogenesis of IBD. Disruption of the intestinal microbiota or dysbiosis may be detrimental in terms of stimulation of the immune system in patients with IBD. It has been shown that dysbiosis is associated with increased intestinal inflammation (148). Antibiotic effects on the gut often lead to symptoms that are indistinguishable from IBD, including diarrhea and abdominal cramping (137). In a large case–crossover study using the General Practice Research Database from 1989 to 1997, exposure to antibiotics within 60 days was associated with a reduced risk of a flare (149). Gut dysbiosis related to antibiotics is associated with C. difficile infection. Patients with IBD have a higher carriage rate of toxigenic C. difficile as compared with controls (150,151). In patients who have an increase in symptoms of diarrhea after antibiotic therapy, concurrent C. difficile infection should be considered and evaluated.
Recommendations.
- Perceived stress, depression, and anxiety, which are common in IBD, are factors that lead to decreased health-related quality of life in patients with Crohn’s disease, and lead to lower adherence to provider recommendations. Assessment and management of stress, depression, and anxiety should be included as part of the comprehensive care of the Crohn’s disease patient (strong recommendation, very low level of evidence).
Many patients associate stress leading to an increase in symptoms of IBD. There appears to be an association between depression and flares in CD activity (152). The somatic symptoms that develop in relationship to depression can cause significant disability. Perceived stress includes issues related to control, disease management, and impact on lifestyle and has a strong relationship to IBD symptoms in multiple studies (137,153,154). The increased bowel symptoms are not always associated with increased inflammation, but may nevertheless contribute to decreased health-related quality of life (154,155,156). CD patients with major depression and anxiety have a greater risk of surgery and a higher degree of health-care utilization than without these comorbidities (157). Children with depression and CD have been shown to have decreased symptomatic disease activity when treated with cognitive behavioral therapy as compared with supportive listening (158).
MANAGEMENT OF DISEASE
General principles
Therapeutic recommendations for patients with CD are established based upon disease location, disease severity, disease-associated complications, and future disease prognosis. Therapeutic approaches are individualized according to the symptomatic response and tolerance to medical intervention. Current therapeutic approaches should be considered a sequential continuum to treat “acute disease” or “induce clinical remission,” and then to “maintain response/remission.” Treatment for active disease should be continued to the point of symptomatic remission or failure to continue improvement. Objective evaluation by endoscopic or cross-sectional imaging should be undertaken to substantiate the subjective improvement of symptoms. The patients’ response to initial therapy should be evaluated within several weeks, whereas adverse events should be monitored closely throughout the period of therapy. In general, clinical evidence of improvement should be evident within 2–4 weeks and the maximal improvement should occur with 12–16 weeks. Patients achieving remission should be considered for maintenance therapy. Those with continued symptoms should be treated with an alternative therapy for mild to moderate disease, have their medication dose adjusted in order to attempt to optimize therapy, or advance to treatment for moderate to severe disease according to their clinical status.
In patients who have active symptoms, despite treatment with a biologic (such as an anti-TNF) it is appropriate to evaluate whether their symptoms result from the presence of active CD with the evaluation of the mucosa with cross-sectional imaging (CTE or MRE) or endoscopy (e.g., colonoscopy). The presence of biomarkers of disease activity can be assessed (such as CRP, fecal calprotectin) but should not exclusively serve as end point for treatment as normalization of the biomarker can occur despite having active mucosal inflammation/ulceration. The presence of mimickers of active IBD such as C. difficile infections, cytomegalovirus infection, and enteric pathogens should be evaluated.
Therapeutic drug monitoring has become very common in the management of CD (159), especially among patients who initially responded to biologic therapy but then developed loss of clinical response, and this approach has been endorsed by several national and international groups (160,161,162). A detailed critical examination of the role of therapeutic drug monitoring was beyond the scope of this guideline. If active CD is documented, then assessment of biologic drug levels and antidrug antibodies (therapeutic drug monitoring) should be considered. There can be three different scenarios explaining biologic failure: mechanistic failure, immune-mediated drug failure, and finally non-immune-mediated drug failure. Individuals who have therapeutic drug levels and no antibodies with the presence of active mucosal ulceration are considered to have mechanistic failure and a medication with another class should be considered (e.g., in a patient on anti-TNF therapy with active inflammation, consideration of anti-IL12/23 therapy or anti-integrin therapy). Non-immune-mediated pharmacokinetic mechanisms occur when patients have subtherapeutic trough concentrations and absent antidrug antibodies. This scenario is a consequence of rapid drug clearance, classically in the setting of a high inflammatory burden. Immune-mediated drug failure is seen in patients who have low or undetectable trough concentrations and high titers of antidrug antibodies. A recent guideline has suggested minimal “therapeutic” target trough levels; infliximab ≥7.5 μg/ml, adalimumab ≥5 μg/ml, and certolizumab pegol ≥20 μg/ml (161).
The following sections review the specific data and recommendations for the treatment of luminal inflammatory CD. The section focusing on fistulizing CD will follow this section. The anatomic distribution and disease activity are the factors to be considered when determining appropriate medical therapy for individual patients with CD. The anatomic distribution of disease is important only for medications with targeted delivery systems, such as sulfasalazine, mesalamine, and enteric-coated budesonide, or where the target for the mechanism of action may be localized, such as greater luminal bacterial concentrations in the colon for antibiotics. For all other agents (parenteral or oral corticosteroids, mercaptopurine, azathioprine, methotrexate, infliximab, adalimumab, certolizumab pegol, natalizumab, ustekinumab, vedolizumab, cyclosporine A, or tacrolimus), therapeutic activity against CD is believed to occur throughout the entire GI tract.
Working definitions of disease activity and prognosis
Since the previous editions of these Practice Guidelines, the working definitions of CD activity have changed and evolved. These end points are consistent with the European Crohn’s and Colitis Organization’s (ECCO) grading of disease activity (163). Individuals are often classified based upon their prognosis and their disease activity. The disease activity comprises a combination of symptoms and endoscopic findings, whereas the prognosis is a compilation of factors predictive of a benign or a more virulent course of disease (mandating surgery and/and resulting in disease-related disability).
Although the majority of clinical trials have utilized CDAI to assess therapeutic outcomes, a more “clinical” working definition for CD activity is valuable for the practicing physician. This enables clinicians to guide therapy in an appropriate manner. It should be stressed that there may be various end points to consider when defining remission.
An individual may be in histologic remission, endoscopic remission, clinical remission, or surgical remission. An individual is in symptomatic remission (usually corresponding to a CDAI score <150) when that patient is asymptomatic or without any symptomatic inflammatory sequelae. Individuals included in this category may have responded to medical therapy or surgical therapy (such as ileocolonic resection) and have no residual active disease (164). Individuals who require the use of conventional corticosteroids to achieve clinical well-being are said to be “steroid dependent” and are not considered to be in remission. This statement is based on the potential for adverse events to accrue in patients on conventional corticosteroids.
Individuals with mild–moderate disease (usually corresponding to a CDAI score 150–220) are ambulatory and able to tolerate oral alimentation without manifestations of dehydration, systemic toxicity (high fevers, rigors, and prostration), abdominal tenderness, painful mass, intestinal obstruction, or >10% weight loss. These individuals do not have severe endoscopic lesions.
Severe endoscopic lesions have been defined in several different manners. There are several scoring systems that assess ulcer size, depth, and distribution including the SES-CD (57) (very large ulcers >2 cm) and the CDEIS (56) (deep vs. shallow) (Supplementary Information online). Allez et al. (165) described the severe endoscopic lesion group as patients with large confluent and deep ulcers that occupy >10% of the surface area of at least 1 segment of the colon.
The SES-CD has been helpful to translate endoscopic activity into clinically meaningful findings that are easy to understand for the clinician. It has been proposed that for SES-CD, remission is 0–2, mild is 3–6, moderate is 7–15, and severe is ≥16. Translating these findings into descriptive terms: mild endoscopic activity would consist of altered vascular pattern and erythema or edema. Moderate endoscopic activity would consist of erosions or superficial ulcers taking up >10% but less than 30% of the surface area, and severe disease as large ulcers >2 cm (57,166).
Individuals who are considered to have moderate–severe disease (usually corresponding to a CDAI score 220–450) are considered to have failed to respond to treatment for mild–moderate disease, or those with more prominent symptoms of fever, significant weight loss, abdominal pain or tenderness, intermittent nausea or vomiting (without obstructive findings), or significant anemia. They typically have moderate to severely active endoscopic mucosal disease.
Finally, those individuals who are considered to have severe/fulminant disease (symptomatically usually corresponding to a CDAI score >450) are patients with persistent symptoms despite the introduction of conventional corticosteroids or biologic agents as outpatients, or individuals presenting with high fevers, persistent vomiting, evidence of intestinal obstruction, significant peritoneal signs such as involuntary guarding or rebound tenderness, cachexia, or evidence of an abscess. They have endoscopic or radiographic evidence of severe mucosal disease.
Recently, there has been a move by regulators to require patient-reported outcomes for regulatory approval of new therapeutic agents for the treatment of patients with CD. The primary end point is to measure an end point that “matters” to patients. The Food and Drug Administration (FDA) is moving away from the use of the CDAI to focus on patient-reported outcomes and separately, objective measures of disease, such as findings on endoscopy (167,168).
Symptom assessment
Individual patients with other conditions may have symptoms indistinguishable from those of patients with active luminal CD. A search should be attempted as a general rule to ascertain whether a patient has symptoms from their CD or other conditions, such as bile salt diarrhea, intestinal infection (e.g., Salmonella, Shigella, Campylobacter, and C. difficile), small intestinal bacterial overgrowth (especially if these have had an ileocolonic resection or have known intestinal strictures), bypass from a fistula (such as a gastrocolic fistula), lactose intolerance, irritable bowel syndrome, anorectal sphincter dysfunction, food intolerance, intestinal obstruction or a stricture, accentuated gastrocolic reflex, a medication-related adverse event (such as diarrhea from an aminosalicylates), or other conditions. Although not specific for CD activity, determination of serum CRP and/or fecal calprotectin is suggested as a useful laboratory correlate with disease activity assessed by the CDAI (169). In addition, it is advocated to assess disease activity by use of cross-sectional imaging with CTE or MRE. In individuals without any observable mucosal inflammation or ulceration, consideration should be given to the aforementioned potential differential diagnostic possibilities. However, it is not necessary to have the complete absence of mucosal inflammation to entertain alternative explanations for specific symptoms or signs; there may be several coexisting conditions.
MEDICAL THERAPY
The forthcoming sections review the specific data and recommendations for the treatment of luminal inflammatory CD. In order to effectively treat luminal CD, the anatomic distribution and disease activity are important factors to be considered. The specific medical therapy selected is based on the location, extent, phenotype, and severity of disease. The anatomic distribution of disease is important only for medications with targeted delivery systems.
General approaches
Medical treatment of CD is usually divided into induction and maintenance therapy. These phases of treatment involve achieving control of inflammation relatively quickly (over 3 months or less) and then sustaining that control for prolonged periods of time (beyond 3 months). Treatment is generally chosen according to the patient’s risk profile and disease severity, with a goal of controlling inflammation and, consequently, symptoms arising from active inflammation. It is important to acknowledge, however, that few clinical trials in CD have incorporated objective outcomes such as endoscopic mucosal healing as a primary outcome. Even the most effective available therapies fail to achieve such hard outcomes in the majority of patients enrolled in clinical trials. Another goal is to prevent the occurrence of disease complications, such as stricture and fistula. Medical therapy may also address some aspects of fistulas in CD; however, little evidence suggests that strictures arising in CD may be treated effectively with medications alone. Medical therapy used to treat CD includes the categories of 5-aminosalicylates (5-ASA), antibiotics, corticosteroids, immunomodulators, and biologics (the anti-TNF agents infliximab, adalimumab, certolizumab pegol; agents targeting leukocyte trafficking, including vedolizumab, natalizumab; and the anti-p40 (anti-IL-12/23) antibody, ustekinumab).
Mild-to-moderately severe disease/low-risk disease
Recommendations.
- Sulfasalazine is effective for treating symptoms of colonic Crohn’s disease that is mild to moderately active and can be used as treatment for this patient population (170–174) (conditional recommendation, low level of evidence).
- Oral mesalamine has not consistently been demonstrated to be effective compared with placebo for induction of remission and achieving mucosal healing in patients with active Crohn’s disease and should not be used to treat patients with active Crohn’s disease (strong recommendation, moderate level of evidence).
- Controlled ileal release budesonide at a dose of 9 mg once daily is effective and should be used for induction of symptomatic remission for patients with mild-to-moderate ileocecal Crohn’s disease (strong recommendation, low level of evidence).
- Metronidazole is not more effective than placebo as therapy for luminal inflammatory Crohn’s disease and should not be used as primary therapy (conditional recommendation, low level of evidence).
- Ciprofloxacin has shown similar efficacy to mesalamine in active luminal Crohn’s disease but has not been shown to be more effective than placebo to induce remission in Crohn’s disease and should not be used as therapy for luminal inflammatory Crohn’s disease (conditional recommendation, very low level of evidence).
- Antimycobacterial therapy has not been shown to be effective for induction or for maintenance of remission or mucosal healing in patients with Crohn’s disease and should not be used as primary therapy (conditional recommendation, low level of evidence).
- For patients with low risk of progression, treatment of symptoms with anti-diarrheals, other nonspecific medications, and dietary manipulation, along with careful observation for inadequate symptom relief, worsening inflammation, or disease progression, is acceptable (175) (strong recommendation, low level of evidence).
When treating patients with CD, the agents chosen to treat the disease are chosen based upon the patient’s clinical presentation and prognosis; that is, the risk of progression of their disease (see “Natural History” section). Disease-related complications include the development of stricturing or penetrating complications in patients with CD. There is a subgroup of patients who rapidly progress to complicated disease behaviors, with stricturing and possible bowel obstruction or internal penetrating fistulas, or both, often resulting in intra-abdominal sepsis. These individuals are in the high-risk group. Risk factors for progression include young age at the time of diagnosis, ileal disease location, serological response to specific microbial antigens, initial extensive bowel involvement, perianal/severe rectal disease, and presence of a penetrating or stenosis disease phenotype at diagnosis (12,176).
Treating the patient with disease on the milder spectrum presents a conundrum. On the one hand, agents proven to be effective in patients with moderate-to-severe disease, such as anti-TNF agents, are undoubtedly effective in mild disease as well, even if such patients were not explicitly studied in randomized controlled trials. On the other hand, the risk of adverse effects and high cost of such agents may not be justifiable in a low-risk population. Unfortunately, few agents studied in milder disease populations have proven to be effective. The desire to avoid overtreating disease and exposing the mild patient to unnecessary risk has led to the widespread utilization of largely ineffective agents whose use cannot be justified by clinical evidence. For example, 5-ASAs remain widely prescribed for the treatment of CD, despite evidence demonstrating their lack of efficacy.
Mesalamine.
5-ASA acts as a topical anti-inflammatory agent that has efficacy within the lumen of the intestine. Although its use in ulcerative colitis is well established and based upon evidence-based criteria, its use in CD is not well established. Oral mesalamine has not been consistently been demonstrated to be effective compared with placebo for induction of remission and achieving mucosal healing in patients with active CD (177,178,179). Sulfasalazine is formulated as combination of a sulfapyridine with 5-ASA; 5-ASA is responsible for the anti-inflammatory property of this drug, whereas sulfapyridine is the carrier that allows 5-ASA to be delivered into the colon. Sulfasalazine (in the doses of 3–6 g daily) is an effective therapy for treatment of symptoms of patients with mild to moderately active colonic CD and/or ileocolonic CD, but not in those with isolated small bowel disease. Sulfasalazine has not been demonstrated to be more effective than placebo for achieving mucosal healing in patients with CD (180,181,182). For rectal and sigmoid disease, 5-ASA suppository and enema preparations are effective for induction and maintenance of remission in patients with ulcerative colitis; however, the role of topical mesalamine in CD, although commonly used, is of limited benefit.
Corticosteroids.
Corticosteroids are used primarily for the treatment of flares of CD. Conventional corticosteroids are effective for reducing the signs and symptoms of active CD and induction of remission in patients with moderately to severely active CD. Oral formulations may be used for mild to moderate disease, whereas systemic corticosteroids are used for moderate to severe disease. Conventional corticosteroids are not consistently effective to enable patients to achieve mucosal healing. They have historically been used as a “bridge” to permit symptom control until immunomodulators and/or biologic agents become effective and enable mucosal healing.
Although not as effective as conventional oral corticosteroids such as prednisone, controlled ileal release (CIR) budesonide may be effective for short-term relief of symptoms of mild-to-moderate CD in patients whose disease is confined to the terminal ileum and right colon. CIR budesonide is a pH-dependent ileal release oral corticosteroid formulation with high topical activity and low systemic bioavailability (∼10–20%). CIR budesonide has been demonstrated to be effective in randomized placebo controlled trials for treatment of active mild-to-moderate ileocecal CD (183,184). The lesser efficacy of CIR budesonide is balanced against the agent’s release profile, limited to the ileum and right colon, and its topical activity with extensive first-pass effect, minimizing systemic exposure to corticosteroid effects.
Antimicrobial therapy.
In patients with CD it is hypothesized that the development of chronic intestinal inflammation is caused by an abnormal immune response to normal flora in genetically susceptible hosts. The involvement of bacteria in CD inflammation has provided the rationale for including antibiotics in the therapeutic armamentarium. The precise mechanisms whereby broad-spectrum antibiotics are beneficial in the treatment of a subset of CD patients are uncertain. Several proposed mechanisms of efficacy include direct immunosuppression (e.g., metronidazole), elimination of bacterial overgrowth, and abolishment of a bacterially mediated antigenic trigger.
Although widely used in the past, the primary role of antibiotics for the treatment of luminal CD is not established. Metronidazole is not more effective than placebo at inducing remission in patients with CD (185,186). Ciprofloxacin has shown similar efficacy to mesalamine in active CD, but has not been shown to be more effective than placebo to induce remission in CD. Neither of these agents has been shown to heal the mucosa in patients with active luminal CD (186,187,188,189). Broad-spectrum antibiotics are used for the treatment of pyogenic complications (e.g., intra-abdominal and mesenteric abscesses) in patients with CD.
Metronidazole may be helpful to prevent postoperative recurrence in CD. Its efficacy is increased over placebo when used in combination with azathioprine. Ornidazole has been more helpful than placebo to prevent postsurgical recurrence of clinical and endoscopic CD. In addition, a novel enteric form of rifaximin may be of benefit for mild-to-moderate CD (190) (see Maintenance section for a detailed description).
The relationship of mycobacterial disease to the development of CD has been extensively evaluated. The absence of mycobacteria in all tissue examined (even when assessed by PCR) and the lack of significant patient disease benefit when treated with multidrug regimens has led to the recommendation that antimycobacterial therapy should not be used to treat patients with active CD. Antimycobacterial therapy has not been shown to be effective for induction or for maintenance of remission or mucosal healing in patients with CD (191,192).
Diet.
Some studies suggest that dietary therapies, including elemental, semielemental, and defined diets, may be effective in some patients with CD, including reduction of objective indicators of mucosal inflammation. These benefits, however, are not durable, with symptoms and active inflammation reoccurring upon resumption of an unrestricted diet. Therefore, dietary therapies may be considered as an adjunct to other therapies in induction therapy (193). Patients deemed to be at low risk for progression of disease may be treated with nonspecific therapies directed at symptoms, but must be followed carefully for signs of disease worsening or progression.
Provided that the goal of treatment is the normalization, or at least substantial improvement, of objective indicators of mucosal inflammation, providers can avoid the pitfall of inadequate disease treatment that, over time, will culminate in progression of disease and the occurrence of important complications even if they choose expectant observation and treatment directed to alleviating symptoms.
Moderate-to-severe disease/moderate-to-high-risk disease
Corticosteroids.
Recommendations
- Oral corticosteroids are effective and can be used for short-term use in alleviating signs and symptoms of moderate to severely active Crohn’s disease (194) (strong recommendation, moderate level of evidence).
- Conventional corticosteroids do not consistently achieve mucosal healing and should be used sparingly (weak recommendation, low level of evidence).
Systemic corticosteroids are ineffective for maintenance therapy in patients with CD. Topical corticosteroids, although commonly used in CD, are of limited benefit (Summary Statement).
Patients experiencing moderate-to-severe symptoms, or who have features of moderate to high risk of progression and complication, require treatment with more effective agents. Conventional corticosteroid treatment, such as prednisone and methylprednisolone given orally or, for more severe disease, intravenous corticosteroids are effective in alleviating signs and symptoms of a flare. However, even short-term use may be accompanied by important adverse events, such as bone loss, mood disorder, insomnia, hypertension, elevated blood glucose, narrow angle glaucoma, acne, weight gain, hypoadrenalism, and other important consequences. The appropriate prednisone equivalent doses used to treat patients with active CD are at doses ranging from 40 to 60 mg/day (195,196). Higher doses, such as 1 mg/kg body weight per day of prednisolone, have also been studied. These doses are typically maintained for 1–2 weeks and tapered at 5 mg weekly until 20 mg and then 2.5–5.0 mg weekly. Corticosteroid tapers should generally not exceed 3 months. Oral prednisone doses or equivalent doses in other oral steroids exceeding 60 mg a day are not recommended. There have been no adequately powered comparative trials between different steroid-tapering regimens in the treatment of patients with CD. Despite their efficacy in reducing signs and symptoms of active CD, nearly 1 in 5 patients will prove to be steroid refractory, and an additional one-third will become steroid dependent, unable to taper without subsequent recrudescence of symptoms. These limitations may be the result of unreliable efficacy in healing of the mucosa, even among those who experience symptomatic relief. In addition, corticosteroids are implicated in the development of perforating complications (abscess and fistula) and are relatively contraindicated in those patients with such manifestations. For all these reasons, corticosteroids should be used sparingly in CD. Once begun, care should be taken to ensure that corticosteroids are successfully discontinued, and steroid-sparing agents should be used.
Immunomodulators.
Recommendations
- Azathioprine (at doses of 1.5–2.5 mg/kg/day) and 6-mercaptopurine (at doses of 0.75–1.5 mg/kg day) are not more effective than placebo to induce short-term symptomatic remission and should not be used in this manner (strong recommendation, low level of evidence).
- Thiopurines (azathioprine, 6-mercaptopurine) are effective and should be considered for use for steroid-sparing in Crohn’s disease (197,198) (Strong recommendation, low level of evidence).
- Azathioprine and 6-mercaptourine are effective therapies and should be considered for treatment of patients with Crohn’s disease for maintenance of remission (strong recommendation, moderate level of evidence).
- Thiopurine methyltransferase (TPMT) testing should be considered before initial use of azathioprine or 6-mercaptopurine to treat patients with Crohn’s disease (strong recommendation, low level of evidence).
- Methotrexate (up to 25 mg once weekly IM or SC) is effective and should be considered for use in alleviating signs and symptoms in patients with steroid-dependent Crohn’s disease and for maintaining remission (199,200) (conditional recommendation, low level of evidence).
Azathioprine, 6-mercaptopurine, or methotrexate (15 mg once weekly) may be used in treatment of active CD and as adjunctive therapy for reducing immunogenicity against biologic therapy (Summary Statement).
In patients with moderate-to-severe CD who remain symptomatic despite current or prior corticosteroid therapy, the thiopurine analogs (6-mercaptopurine and azathioprine) may be used. Mercaptopurine, and its prodrug, azathioprine, are effective steroid-sparing agents in CD. Methotrexate, when given subcutaneously (SC) or intramuscularly (IM), is also effective as a steroid-sparing agent, but when prescribed to women with child-bearing capability, should be administered only if highly effective contraception is in place. Additionally, men should be counseled to avoid conceiving during use of and within 3 months of stopping methotrexate because of concerns about on effects on spermatogenesis and teratogenicity (201). Thiopurine agents and methotrexate are not effective agents for short-term induction in active, symptomatic disease because of their relatively slow onset of action, between 8 and 12 weeks. The use of methotrexate in combination with steroids is effective for treatment of moderately active steroid-dependent/resistant CD (202,203,204). Azathioprine (at maximal doses of 1.5–2.5 mg/kg/day), 6-mercaptopurine (at maximal doses of 0.75–1.5 mg/kg day), or methotrexate (15–25 mg SC/IM once weekly) may be used in treatment of active CD (198,205,206). These agents can be used as adjunctive therapy for reducing immunogenicity against biologic therapy (6-mercaptupurine or azathioprine typically at reduced doses and methotrexate 12.5–15 mg orally once weekly) (207,208).
A disadvantage of the thiopurine analogs and methotrexate is the slow time to clinical response that may not be evident for as long as 12 weeks. Azathioprine and 6-mercaptopurine are not more effective than placebo to induce remission; they are, however, effective therapies for maintenance of remission in patients with CD. TPMT testing should be considered before initial use of azathioprine or 6-mercaptopurine to treat patients with CD (209,210).
The adverse effects of azathioprine and 6-mercaptopurine include allergic reactions, pancreatitis, myelosuppression, nausea, infections, hepatotoxicity, and malignancy, especially nonmelanoma skin cancer and lymphoma (211,212). Methotrexate has similar adverse effects including nausea and vomiting, hepatotoxicity, pulmonary toxicity, bone marrow suppression and skin cancer, and likely lymphoma; however, an escalated risk of lymphoma has not been conclusively demonstrated in patients with CD. The white blood cell count and liver chemistries should be routinely monitored during their use.
Cyclosporine, tacrolimus, and mycophenolate mofetil therapy have not been shown to be effective for treatment of active luminal CD (213,214,215).
Anti-TNF agents.
Recommendations
- Anti-TNF agents (infliximab, adalimumab, certolizumab pegol) should be used to treat Crohn’s disease that is resistant to treatment with corticosteroids (216,217,218,219,220) (strong recommendation, moderate level of evidence).
- Anti-TNF agents should be given for Crohn’s disease refractory to thiopurines or methotrexate (216,217,218,219,220) (strong recommendation, moderate level of evidence).
- Combination therapy of infliximab with immunomodulators (thiopurines) is more effective than treatment with either immunomodulators alone or infliximab alone in patients who are naive to those agents (221) (strong recommendation, high level of evidence)
The anti-TNF antibodies (infliximab, adalimumab, and certolizumab pegol) are effective for treatment of patients with CD who respond inadequately to treatment with corticosteroids, thiopurines, and methotrexate. In addition, combination therapy of infliximab with immunomodulators is more effective than either agent given alone in patients with no prior exposure to either treatment, suggesting an important synergistic effect. Combination therapy of adalimumab or certolizumab pegol with an immunomodulator has not been well studied, but is likely to be superior in efficacy to therapy with the anti-TNF agent alone, given the immunogenicity of all biologics, and the ability of immunomodulators to reduce the rate of anti-drug antibody formation. Direct evidence supporting the continuation of an immunomodulator (relating to augmented efficacy) when an anti-TNF antibody is begun after failure of the immunomodulator is lacking. Continuing combination therapy in that situation may be considered when it is important to prevent anti-drug antibody formation because of significant disease.
Monoclonal antibody therapy directed against TNF-α has been shown to be more effective than placebo for induction of response, remission, and complete and partial mucosal healing in patients with CD (222,223). These agents are rapid in onset of effect, with benefit often noted within 2 weeks of initiating therapy. Treatment with anti-TNF agents appears to be more effective when given earlier in the course of disease; rates of response and remission are higher if given within 2 years of onset of disease. Anti-TNF-α therapies include infliximab (Remicade), a chimeric mouse-human IgG1 monoclonal antibody that is approved to treat moderate-to-severe CD and fistulizing CD that have failed to respond to conventional therapy. Adalimumab (Humira) and certolizumab pegol (Cimzia) have been approved to treat moderate-to-severe CD that has failed to respond to conventional therapy. These biologic agents are effective for treating patients with CD who have objective evidence of active disease treated with steroids, steroid dependent or refractory to corticosteroids when used alone or in combination with thiopurines (azathioprine or 6-mercaptopurine) or methotrexate. Certolizumab pegol is a PEGylated Fab fragment to TNF-α and adalimumab is a fully human IgG1 monoclonal antibody directed against TNF-α; both of these agents are self-administered SC. Combination therapy with infliximab and azathioprine is more effective than monotherapy with either azathioprine or infliximab alone for achieving response, remission, steroid-free remission, and mucosal healing (221). Combination therapy is the preferred strategy of treatment for patients with CD who do not have risk factors precluding its use.
Anti-TNF therapy has also been shown to lessen postoperative endoscopic recurrence. Before anti-TNF therapy is considered for use in patients with CD, risk vs. benefit needs to be assessed in each individual patient, given the potential risk for infection and malignancy with their use.
Before initiation of anti-TNF therapy, assessment for latent and active tuberculosis and other latent opportunistic infections such as histoplasmosis and blastomycosis when potentially present should be initiated (including evaluation of history of epidemiological risk factors, physical examination, chest radiography, tuberculin skin tests, and interferon-γ release assays). Interferon-γ release assays are likely to complement the tuberculin skin test and are preferred in patients who are Bacillus Calmette-Guerin (BCG) vaccinated, if available. Similar testing and therapy should also be considered before corticosteroids or other immunomodulators in patients at high risk of tuberculosis. If latent tuberculosis is detected, initiation of chemoprophylaxis with anti-tuberculous therapy should be initiated for several weeks or months before administration of anti-TNF therapy. It may be appropriate to consider a second tuberculin skin test in an immunocompromised host after the initial test is negative. This is classically done 1 to 3 weeks later (224).
Assessment for the presence of viral hepatitis (hepatitis B surface antigen, hepatitis B surface antibody and hepatitis B core antibody) should be performed in all CD patients before the initiation of anti-TNF therapy. If a patient is seronegative for hepatitis B, vaccination (using a recombinant vaccine) should be initiated, ideally before the introduction of biologic therapy. Assessment of serologic response is advocated after vaccination. Before and during treatment with biologic and/or immunomodulator therapy, patients who are HBsAg (hepatitis B surface antigen)-positive carriers should receive treatment with antiviral agents (nucleoside/nucleotide analogs) in order to avoid hepatitis B flare and liver failure.
Other appropriate vaccinations (pneumococcal polysaccharide vaccine (including PSV-13 and PPSV-23), varicella, human papilloma virus, inactivated influenza vaccine, hepatitis A vaccine, and herpes zoster) should be initiated ideally before use of biologic therapy. The use of live attenuated vaccines should be avoided in IBD patients using immunomodulator therapy or biologic therapy (e.g., measles–mumps–rubella, vaccinia, yellow fever, live attenuated influenza vaccine, varicella, oral polio, and BCG). Vaccination status ideally should be reviewed and updated at diagnosis. Live vaccines should be avoided after initiation of systemic immune suppressive therapy (225).
The safety profile in randomized controlled studies of biological agents is generally favorable, but a few patients may experience severe side effects. Individuals at increased risks for use of anti-TNF therapy include patients with prior demyelinating disorders (e.g., optic neuritis and multiple sclerosis), patients with congestive heart failure, and individuals who have had prior lymphoma or known malignancies. Infectious complications may occur with the use of these agents, and thus vigilance is advocated when treating these patients (226).
Biosimilar anti-TNF agents
Biosimilar infliximab and biosimilar adalimumab are effective treatments for patients with moderate-to-severe Crohn’s disease and can be used for de novo induction and maintenance therapy (Summary Statement).
Insufficient data exist to support the safety and efficacy of switching patients in stable disease maintenance from one biosimilar to another of the same biosimilar molecule (Summary Statement).
There are currently biosimilars for infliximab (infliximab-dyyb, CT-P13 (Inflectra Pfizer, Remsima Celltrion), infliximab-abda (Renflexis, Merck and Samsung Bioepsis), Infliximab-qbtx (Ixifi, Pfizer) and adalimumab as adalimumab-atto (Amjevita, Amgen) as well as adalimumab-adbm (Cyltezo, Boehringer Ingelheim) that have gained regulatory approval for use in patients with CD. Unlike the generics of small-molecule drugs, exact replicas cannot be made of biologics because of their structural complexity and complicated manufacturing process. Their amino acid sequences remain the same but they may differ in their glycosylation patterns. It is important to recognize that different patterns in glycosylation influence a molecule’s solubility, stability, clearance, immunogenicity, and immune effector function. Thus, it is important to stress that biosimilars differ from small-molecule generics. A biosimilar is a biological product that is highly similar to the reference product notwithstanding minor differences in clinically inactive components; there are no clinically meaningful differences between the biosimilar product and the reference product in terms of safety, purity, and potency. The biosimilar must have the same strength and dosage form (injectable, for example) and route of administration as the reference product. The approval pathway for biosimilars differs from that of the originator biologic—the primary emphasis is on analytical characterization, preclinical/animal studies, and pharmacokinetic studies. Once these have been demonstrated, clinical studies demonstrating pharmacokinetics, efficacy, and safety that are similar to the originator biologic in one indication for which the drug is approved are often sufficient for extrapolation to all indications. Interchangeable biosimilars represent agents that are similar to the US licensed reference product that are expected to produce the same clinical result to the reference product in any given patient, even after multiple switches between the reference and biosimilar products. If a product is indicated for multiple administrations, then the product must be able to be alternated with the reference product without any loss of efficacy or change in risk of adverse effects. An interchangeable biosimilar can be substituted at the pharmacy level without the intervention of a health-care provider. Interchangeability is a federal designation that may or may not be followed at the state level, and this is where the substitution laws can vary from state to state. The ability of a pharmacist to substitute a biosimilar for an innovator drug will be determined by each state’s pharmacy board, not by the FDA interchangeability designation.
Despite the potential advantages of cost savings and improved patient access with biosimilars, there exist concerns by some that small differences in the efficacy and safety of these molecules may be magnified in less anti-TNF-responsive diseases such as IBD, leading to altered immunogenicity and drug metabolism. A large randomized, non-inferiority phase 4 trial of patients with CD, ulcerative colitis, spondyloarthritis, rheumatoid arthritis, psoriatic arthritis, and plaque psoriasis showed that switching from infliximab originator to CT-P13 (biosimilar) was not inferior to continued therapy with the originator (224).
There are no data guiding physicians on whether we can switch from an innovator biologic to a biosimilar if mandated, and then switch back to the innovator if clinically necessary or whether there are changes in contractual arrangements. In addition, the role of potentially using immunomodulators to lessen immunogenicity requires further assessment.
Agents targeting leukocyte trafficking.
Recommendations
- For patients with moderately to severely active CD and objective evidence of active disease, anti-integrin therapy (with vedolizumab) with or without an immunomodulator is more effective than placebo and should be considered to be used for induction of symptomatic remission in patients with Crohn’s disease (strong recommendation, high level of evidence).
- Natalizumab is more effective than placebo and should be considered to be used for induction of symptomatic response and remission in patients with active Crohn’s disease (strong recommendation, high level of evidence)
- Natalizumab should be used for maintenance of natalizumab-induced remission of Crohn’s disease only if serum antibody to John Cunningham (JC) virus is negative. Testing for anti-JC virus antibody should be repeated every 6 months and treatment stopped if the result is positive (227,228) (strong recommendation, moderate level of evidence).
Inhibitors of leukocyte trafficking recently have expanded the therapeutic options for patients with CD. Natalizumab, an anti-α4 integrin antibody, broadly interferes with leukocyte trafficking systemically and inhibits binding to both vascular cell adhesion molecule-1 and mucosal addressin cell adhesion molecule-1. Although effective in patients who have failed other agents, the risk of progressive multifocal leukoencephalopathy (PML), caused by JC virus, is as high as 1 in 100 among patients with JC virus antibody positivity, prior use of immunosuppressive agents, and 2 or more years of use. Treatment with natalizumab is best limited to those patients who are not seropositive for anti-JC virus antibody that should be checked before initiating therapy and at minimum every 6 months thereafter.
In contrast, vedolizumab (Entyvio) selectively inhibits α4β7 integrin interaction with mucosal addressin cell adhesion molecule-1, making it relatively specific for leukocyte trafficking to the gut. This agent has historically been used in adult patients with moderately to severely active CD who have had an inadequate response with, lost response to, or were intolerant to a TNF blocker or immunomodulator, or had an inadequate response with, were intolerant to, or demonstrated dependence on corticosteroids. To date, no cases of PML have been reported with the use of vedolizumab that is effective for patients who have active, symptomatic CD despite treatment with corticosteroids, thiopurines, methotrexate, or anti-TNF agents. This agent has been used to achieve clinical response, clinical remission, and corticosteroid-free remission (229,230,231,232). It is important to also recognize that this medication can also be positioned before use of these agents and failure of other agents is not mandatory or advocated. For patients with moderately to severely active CD and objective evidence of active disease, vedolizumab, with or without an immunomodulator, is more effective than placebo for induction of response, remission, and achieve mucosal healing. The onset of the clinical effect of vedolizumab may be slower than with anti-TNF agents in CD. Patients who have received prior treatment with anti-TNF agents in particular require longer treatment, with efficacy rates at 10 weeks equaling those of anti-TNF-naive patients at 6 weeks. As with all biologic agents, concomitant therapy with an immunomodulator reduces rates of anti-vedolizumab antibodies. However, prospective clinical trials comparing therapeutic strategies of vedolizumab monotherapy with combination therapy with an immune modulator have not been reported. A recent network meta-analysis suggests that adalimumab or combination therapy with infliximab and azathioprine is more effective than vedolizumab in inducing and maintaining remission in CD (206).
Agents targeting IL-12/23 (anti-p40 antibody).
Recommendations
- Ustekinumab should be given for moderate-to-severe Crohn’s disease patients who have failed previous treatment with corticosteroids, thiopurines, methotrexate, or anti-TNF inhibitors, or who have had no prior exposure to anti-TNF inhibitors (233) (strong recommendation, high level of evidence).
Ustekinumab, an anti-p40 antibody that inhibits IL-12 and -23, is efficacious in patients with CD whose prior treatments have included corticosteroids, immunomodulators, or anti-TNF agents. Stated another way, efficacy for induction of remission has been demonstrated in both the anti-TNF-failure and conventional therapy-failure populations (233). An extensive safety database in patients with psoriasis demonstrates an excellent safety profile, without apparent increase in serious infections or malignancies (234). This favorable safety profile appears consistent with data from clinical trials of ustekinumab in CD, although with less accumulated long-term exposure, and despite higher doses being used. No head-to-head studies have yet directly compared the efficacy of ustekinumab with vedolizumab or with anti-TNF agents. Lacking such data, the choice of first biologic is at the discretion of the provider and patient according to individual risk–benefit preferences.
Other medications.
Recommendations
- Cyclosporine, mycophenolate mofetil, and tacrolimus should not be used for Crohn’s disease (213,235,236,237,238,239,240,241) (strong recommendation, moderate level of evidence).
Despite its efficacy in ulcerative colitis, cyclosporine has not been demonstrated to be effective in CD. Tacrolimus, another calcineurin inhibitor, has been studied only in small, uncontrolled case series, with some suggestion of benefit for luminal disease (239,241). In addition, mycophenolate mofetil, an inhibitor of inosine monophosphate dehydrogenase, has not been shown to be efficacious in CD. Thalidomide may be effective in severe CD, but should be used only in exceptional circumstances, given the high risk of serious adverse effects that include sedation, constipation, peripheral neuropathy, and severe birth defects (242).
Severe/fulminant disease
Recommendations.
- Intravenous corticosteroids should be used to treat severe or fulminant Crohn’s disease (243) (conditional recommendation, moderate level of evidence).
- Anti-TNF agents (infliximab, adalimumab, certolizumab pegol) can be considered to treat severely active Crohn’s disease (216,217,218,219,220) (strong recommendation, moderate level evidence).
- Infliximab may be administered to treat fulminant Crohn’s disease (conditional recommendation, low level of evidence).
Although not well studied, intravenous corticosteroids are deemed to be effective for more severe or fulminant disease in the hospitalized patient. Parenteral methylprednisolone is effective for acute treatment of severe disease, with doses from 40 to 60 mg/day. An additional use of corticosteroids is in preventing anti-drug antibodies by administering as a bolus before infusion of infliximab. Pivotal trials of infliximab, adalimumab, and certolizumab pegol included patients with moderate-to-severe disease activity as indicated by the CDAI. These agents may be effective in patients with severe disease; however, it should be noted that patients with the most severe symptomatic disease, generally with CDAI scores greater than 450, were excluded. Clinical experience suggests that some patients with the most severely symptomatic inflammatory CD may respond to TNF inhibition. For more fulminant cases, infliximab may be effective, whereas the efficacy of adalimumab and certolizumab pegol in such cases is less certain. This may, in part, be attributed to the weight-based dosing used for infliximab that leads to generally higher doses than with adalimumab and certolizumab pegol, and that may be more effective when there is a higher burden of inflammation.
FISTULIZING CROHN’S DISEASE
Perianal/fistulizing disease
Recommendations.
- Infliximab is effective and should be considered in treating perianal fistulas in Crohn’s disease (244,245) (strong recommendation, moderate level of evidence).
- Infliximab may be effective and should be considered in treating enterocutaneous and rectovaginal fistulas in Crohn’s disease (245,246) (strong recommendation, moderate level of evidence).
- Adalimumab and certolizumab pegol may be effective and should be considered in treating perianal fistulas in Crohn’s disease (247,248) (strong recommendation, low level of evidence).
- Thiopurines (azathioprine, 6-mercaptopurine) may be effective and should be considered in treating fistulizing Crohn’s disease (198) (strong recommendation, low level of evidence).
- Tacrolimus can be administered for short-term treatment of perianal and cutaneous fistulas in Crohn’s disease (240) (strong recommendation, moderate level of evidence).
- Antibiotics (imidazoles) may be effective and should be considered in treating simple perianal fistulas (249) (strong recommendation, moderate level of evidence).
- The addition of antibiotics to infliximab is more effective than infliximab alone and should be considered in treating perianal fistulas (250) (strong recommendation, moderate level of evidence).
- Drainage of abscesses (surgically or percutaneously) should be undertaken before treatment of fistulizing Crohn’s disease with anti-TNF agents (251) (expert opinion) (conditional recommendation, very low level of evidence).
- Placement of setons increases the efficacy of infliximab and should be considered in treating perianal fistulas (251,252) (strong recommendation, moderate level of evidence).
The presence of a perianal abscess in CD should prompt surgical drainage (Summary Statement).
Fistulizing CD is a therapeutic challenge that requires careful evaluation and coordination of care between medical and surgical providers in order to direct therapy appropriately.
Fistulas occur in approximately one-third of patients with CD, with perianal fistulas representing the most common location. Internal fistulas rarely require therapy and are often asymptomatic. If fistulas occur and they are symptomatic and represent major fistulas (stomach to ileum; mid or proximal small bowel to colon) and are associated with diarrhea or small intestinal bacterial overgrowth, then surgery or medical therapy is advocated. Before initiation of immunosuppressive therapy with agents such as biologic therapy or antimetabolite therapy (azathioprine, 6-mercaptopurine, or methotrexate), pyogenic complications such as abscess should be excluded with cross-sectional imaging. If abscesses are present they should be treated initially with drainage before initiation of biologic therapy or immunosuppression (253).
Small (<5 mm) abscesses may not require surgical drainage. For asymptomatic simple perianal fistulas, no treatment is required. Symptomatic simple fistulas may be treated with noncutting setons or fistulotomy. Complex fistulae with or without abscess should be treated with seton placement (254), typically in combination with appropriate medical therapy. The timing of seton removal depends on subsequent therapy and drainage of abscess. A surgical advancement flap may close simple fistula or complex fistula, for example rectovaginal fistula, in the setting of no active infection or inflammation (255,256,257).
The presence of high-output fistulas typically mandates surgical intervention (proximal bowel diversion, bowel segment resection, or surgical fistula closure) and historically do not close spontaneously or with medical therapy. Low-output fistulas may be treated with antimetabolite therapy or biologic therapy alone or in combination with each other; however, the evidence supporting the use of anti-metabolite is not very robust. In addition, these agents can be used individually or in combination with antibiotics.
When assessing patients with perianal fistulas (the most common fistula location in patients with CD) we categorize the fistulas as either simple (located distal to the dentate line primarily in the anal sphincter region with a single track) or complex. A complex fistula can be transsphincteric, suprasphincteric, and intersphincteric in its location and may have multiple fistula tracts. This classification is important to perform as treatments may differ among these categories.
In the absence of active mucosal involvement in the rectum, patients with simple fistulas who have CD may respond well to fistulotomy or mucosal advancement flap surgery, whereas patients with mucosal involvement may benefit from seton placement rather than fistulotomy. Consideration may also be given to immunomodulators, vedolizumab, or anti-TNF-α agents, with the best evidence supporting the efficacy of infliximab.
The optimal management of complex perianal fistulas should include a combination of surgery with an anti-TNF. The surgery involves an exam under anesthesia with identification of abscesses and fistula tracts. The pelvic sepsis related to fistula abscesses leads to tissue destruction of the tissue, anal sphincter, and more extensive perianal, gynecologic, and genitourinary complications. To that end, any fistula with an abscess or complex fistula (i.e., involving the anal sphincter, vagina, or multiple tracts) should be drained of infection. Setons are the most common method to allow for continued drainage of infection and inflammatory fistula tracts and should be performed before initiation of immunosuppression (258). Several studies have shown the benefit of placement of setons followed by infliximab. The combination of a seton with infliximab has demonstrated a better overall fistula healing response, longer duration of fistula closure and prevention of repeated abscess, and lower overall fistula recurrence rate (252,259,260). In the setting of significant refractory disease a proximal diversion to enable rectal and/or perianal healing may be necessary. After the diversion, initiation of a new therapy such as anti-TNF therapy with or without an immunomodulator additionally may promote healing of the perineal disease. However, a systematic review suggests that the long-term success of diverting ostomy for perianal CD is very low (261). In very severe clinical scenarios, proctectomy or total proctocolectomy with permanent stoma may be necessary. Surgical advancement flaps play a role in the improvement of long-term healing rates in combination with an anti-TNF (262).
Internal fistulas remain more difficult to treat. Internal fistulas may occur in the form of rectovaginal fistulas, enterovesical (or colovesical) fistulas, or enteroenteric fistulas. Appropriate management of rectovaginal fistulas classically entails use of medical therapy with immunomodulator therapy (monotherapy with azathioprine/6-mercaptopurine or anti-TNF antibody or combination therapy with both) as initial treatment. This treatment regimen is usually considered before surgery. The goal of medical therapy is to heal the inflamed bowel mucosa and then subsequently to enable surgical intervention. Surgical options for the treatment of rectovaginal fistulas might include excision of the fistula and the interposition of healthy tissue between the rectum and vagina. In general, the surrounding tissues are best when not inflamed. The presence of any active infection should be treated and resolved before attempting repair. After fistula excision the treatment with a mucosal advancement flap can then be performed. In a similar manner, enterovesical or colovesical fistulas may be treated with immunomodulator therapy or anti-TNF antibodies, or both, but the occurrence of recurrent symptomatic urinary tract infection is a relative indication for surgery (especially if associated with pyelonephritis). Surgery usually involves resection of involved inflamed bowel and closure of the bladder defect.
Finally, enteroenteric fistulas (such as ileum to ileum) may be present and asymptomatic. As these fistulas are asymptomatic they do not require surgical management; however, treatment with immunomodulator therapy or anti-TNF antibodies, or both, might be initiated. Major symptomatic internal fistulas, such as gastrocolic and coloduodenal fistulas, may cause symptoms as they bypass part of the intestine. If medical management fails or if an abscess develops, surgical intervention is recommended.
A variety of different medications have been used to treat fistulas in patients with CD. Mesalamine and corticosteroids are ineffective treatments for fistulizing CD.
Although poorly studied, antibiotics may heal simple, superficial perianal fistulas, with minimal penetration of sphincter musculature, and play an adjunctive role in treating perianal sepsis associated with more complex fistulas. Simple fistulas respond well to medical therapy. Metronidazole and ciprofloxacin have been evaluated in the management of perianal CD (263,264,265,266). Typical initial medical therapy might include therapy with metronidazole (10 to 20 mg/kg/day orally for 4 to 8 weeks) and/or ciprofloxacin (500 mg orally twice daily for 4 to 8 weeks) or levofloxacin (500–750 mg once daily for 4 to 8 weeks) for the fistula and treatment of concurrent mucosal disease. Antibiotics (e.g., metronidazole, ciprofloxacin, and levofloxacin) improve fistula symptoms and may be associated with healing of simple fistulas. Metronidazole and ciprofloxacin have not been effective at healing complex perianal fistulas, but may improve symptoms related to the fistula (249). Antibiotics are most commonly administered for active infection, but rarely replace the need for surgical drainage of an abscess. There have been recent warnings for the occurrence of tendonitis, tendon rupture, and neuropathy when using the fluoroquinolones.
Thiopurines, although poorly studied, may also lead to reduction of the symptoms of perianal fistulas, but can be slow in onset of effect. Azathioprine and 6-mercaptopurine have been shown to be effective for treating fistulizing CD. Tacrolimus is effective for short-term treatment of fistulizing CD; however, significant toxicity precludes long-term therapy with this agent
The anti-TNFs are effective for closure of perianal fistula, but only infliximab has been studied in a prospective, randomized controlled trial. In the initial study, infliximab 5 mg/kg at 0, 2, and 6 weeks led to cessation of all drainage of perianal fistula on 2 consecutive visits 1 month apart, defined as complete closure, in the majority of patients.(244) A subsequent, large randomized controlled trial confirmed the efficacy of infliximab for induction of closure of perianal fistula, but also every 8 week dosing at 5 mg/kg for maintenance of complete closure and response, defined as >50% closure on clinical assessment (245). Infliximab may also be effective at maintaining response of rectovaginal fistula closure (246). Subsequent studies from clinical practice cohorts have replicated the efficacy of infliximab for the induction of perianal fistula closure and maintenance of response (267,268). Although not as thoroughly studied, adalimumab may also be effective in treating signs and symptoms of perianal fistulas. Perianal fistula closure was not a primary end point of any of the adalimumab or certolizumab studies. On post hoc analysis from two adalimumab CD studies, there was no benefit over placebo for fistula closure (269,270). In a large maintenance study of adalimumab for CD, fistula response and remission was a secondary end point that was achieved in a higher percentage of patients compared with placebo (218,220,271,272). A small open-label trial of adalimumab also suggested a benefit for fistula induction of remission and maintenance of closure (272). Similarly, there is a suggestion of efficacy based upon post hoc analysis of certolizumab pegol, vedolizumab, and ustekinumab trials, but no controlled studies indicating unequivocal benefit in fistulizing CD (220,273,274). In addition, the use of combination therapy with anti-TNF therapy and antibiotics may be more beneficial than each agent individually. Combination therapy with ciprofloxacin and infliximab or ciprofloxacin and adalimumab has been shown to be more effective than monotherapy for each anti-TNF agent to treat fistulas and is effective in reduction of fistula drainage.
MAINTENANCE THERAPY OF LUMINAL CROHN’S DISEASE
No maintenance treatment is a treatment option for some patients with asymptomatic (silent), mild Crohn’s disease (Summary Statement).
Surgery may be considered for patients with symptomatic Crohn’s disease localized to a short segment of bowel (Summary Statement).
Recommendations
- Once remission is induced with corticosteroids, a thiopurine or methotrexate should be considered (strong recommendation, moderate level of evidence).
- Patients who are steroid dependent should be started on thiopurines or methotrexate with or without anti-TNF therapy (strong recommendation, moderate level of evidence).
Corticosteroids are not indicated for long-term treatment of CD because of lack of efficacy for maintenance of remission and adverse effects (275). There are three scenarios by which a thiopurine is used after corticosteroid induction of remission. One scenario is to initiate the thiopurine at the time of the first course of corticosteroid, the second is after repeated courses of corticosteroids or in patients who are corticosteroid dependent (i.e., unable to taper the steroid without CD relapse), and the third is as a concomitant medication to an anti-TNF. The efficacy of 6-mercaptopurine 1.5 mg/kg/day as a maintenance medication when administered in combination with the first course of corticosteroid for newly diagnosed pediatric CD is good (276). Presumably, the same efficacy would be realized with azathioprine in an adult population, but a randomized open-label study of early use of azathioprine in CD was unable to demonstrate a benefit with respect to time in clinical remission (277). The most common scenario for maintenance of remission with a thiopurine is that of a corticosteroid-dependent patient. There are several studies that have demonstrated that azathioprine 2.5 mg/kg/day and 6 mercaptopurine 1.5 mg/kg/day are effective for the maintenance of remission in CD (181,278,279,280,281,282). The combination of a thiopurine with an anti-TNF will be discussed separately in the “Anti-TNF maintenance” section. Methotrexate is also effective as a corticosteroid-sparing agent for the maintenance of CD remission (283,284). Parenterally (SC or IM) administered methotrexate at a dose of 25 mg per week is effective for maintenance of remission in CD after steroid induction (285). If steroid-free remission is maintained with parenteral methotrexate at 25 mg per week for 4 months, the dose of methotrexate may be lowered to 15 mg per week (204). Data demonstrating efficacy of the use of oral methotrexate for maintenance of remission in patients with CD are lacking. It is perceived that patients with normal small bowel absorption may be started on or switched from parenteral to oral methotrexate at 15 mg to 25 mg once per week; however, controlled data evaluating this contention are lacking. Similarly, a low dose of oral methotrexate (12.5 mg once per week) has been demonstrated to be effective at preventing immunogenicity to a monoclonal antibody biologic agent.
Recommendations
- Oral 5-aminosalicylic acid has not been demonstrated to be effective for maintenance of medically induced remission in patients with Crohn’s disease, and is not recommended for long-term treatment (strong recommendation, moderate level of evidence).
Data are lacking demonstrating the effectiveness of sulfasalazine or of olsalazine for the maintenance of medically induced remission in patients with Crohn’s disease and these agents are not recommended for long-term treatment (Summary Statement)
5-Aminosalicylates have been extensively studied for maintenance of medically induced remission of CD and have shown limited benefit. There were 11 placebo-controlled trials ranging in doses between 1 and 4 g per day and the duration of maintenance treatment between 4 months and 36 months, with most evaluated 12-month duration (286,287,288,289,290,291,292,293,294,295,296). Four of the studies reported a significant decrease in CD relapse compared with placebo (P<0.05); however, the other 7 studies showed no prevention of relapse. There were 5 meta-analyses evaluating the efficacy of mesalamine for the maintenance of medically induced remission in patients with CD (173,297,298,299,300). The number of trials evaluated in the meta-analyses ranged from 7 to 10 with a total of 941 patients to 1,500 patients in each analysis. Although most of the meta-analyses showed a clinically significant benefit of mesalamine for maintenance of remission, the 95% CI for the odds ratio either crossed unity or approached unity. The therapeutic advantage between mesalamine and control was <10% for most meta-analyses with a number needed to treat (NNT) over 15. Given the totality of data, 5-ASA is not recommended for maintenance of medically induced remission.
Recommendations
- Corticosteroids are not effective for maintenance of medically induced remission in Crohn’s disease and should not be used for long-term treatment (strong recommendation, moderate level of evidence).
- Budesonide should not be used to maintain remission of Crohn’s disease beyond 4 months (strong recommendation, moderate level of evidence).
Corticosteroids are effective for induction of remission of CD but are not effective for maintenance. The use of corticosteroids should not exceed 3 continuous months without attempting to introduce corticosteroid-sparing agents (such as biologic therapy or immunomodulators). In a meta-analysis including 403 patients with surgically or medically induced remission, corticosteroids were not effective at maintaining remission (275) The rates of remission were no different between placebo and corticosteroids at 6, 12, and 24 months. The adverse events associated with corticosteroids were significantly higher than placebo at all time points and should not be used for maintenance of remission. Enteric-coated budesonide has been demonstrated to prolong the time to recurrence of symptoms for patients with mild-to-moderate ileocecal CD, but has not been shown to be effective at maintenance of remission. There were six randomized placebo-controlled studies evaluating maintenance of remission of budesonide (301,302,303,304,305,306). The 12-month relapse rates for 3 to 6 mg budesonide ranged from 40 to 74% and were not significantly different than placebo. One study did show a reduction in the relapse rate compared with placebo, but this occurred at an early time point of 3 months (304). Four meta-analyses have been published on the efficacy of budesonide for maintenance of remission in CD. The results are mixed with most showing no benefit in maintenance of remission with only slight improvements in mean time to symptom relapse (307,308,309,310). The budesonide meta-analyses included doses of budesonide at 3 and 6 mg and reported increased adverse events compared with placebo. Abnormal adrenocorticoid stimulation tests and alteration in bone mineral density were higher in budesonide compared with placebo but lower than conventional glucocorticosteroids.
Recommendations
- Anti-TNF therapy, specifically infliximab, adalimumab, and certolizumab pegol, should be used to maintain remission of anti-TNF-induced remission (strong recommendation, high level of evidence).
- Anti-TNF monotherapy is effective at maintaining anti-TNF-induced remission, but because of the potential for immunogenicity and loss of response, combination with azathioprine/6-mercaptopurine or methotrexate should be considered (strong recommendation, moderate level of evidence).
Infliximab, adalimumab, and certolizumab pegol are effective for maintenance of medically induced remission of luminal CD, and numerous clinical trials have supported the use of anti-TNFs beyond induction (218,219,273,311,312,313,314). There has been one meta-analysis and one Cochrane Database Systematic review evaluating anti-TNFs for maintenance of remission (315). In the meta-analysis, CD patients who responded to induction anti-TNF were more likely to maintain remission through 52 weeks with an anti-TNF compared with placebo. The safety of maintenance anti-TNF therapy was also evaluated. There were 21 studies evaluated with a total of 5,356 individuals, and anti-TNF therapy did not increase the risk of serious infection, malignancy, or death compared with placebo. In the Cochrane Database review, the pooled analysis of 5 or 10 mg/kg infliximab every 8 weeks was found to be superior to placebo for maintenance of remission and clinical response to week 54, 400 mg certolizumab pegol every 4 weeks was superior to placebo for maintenance of remission and clinical response to week 26, and 40 mg adalimumab every other week or every week was superior to placebo for maintenance of clinical remission to week 54 (217). Adverse events were equal between anti-TNF therapy and placebo, but the authors noted lymphoma and tuberculosis at higher rates in certain individual trials.
Combination therapy with an anti-TNF and an immunomodulator has been demonstrated to improve short-term efficacy compared with monotherapy (221). The combination of a thiopurine or methotrexate with anti-TNF therapy reduces immunogenicity and the authors recommend this strategy (316,317). Some evidence suggests that immunogenicity may be avoided in monotherapy simply by maintaining robust trough levels of biologic therapy at all times, and that the primary effect of immunomodulator in combination therapy is in nonspecifically increasing trough biologic concentrations (318).
The benefits and risks of combination therapy must be individualized. There is a higher risk of lymphoma in patients treated with azathioprine or 6 mercaptopurine, especially among males and those patients diagnosed at younger ages (197). There is also a rare but increased risk of hepatosplenic T-cell lymphoma that has been reported when a thiopurine is combined with an anti-TNF (319). There is no higher risk of opportunistic infections with the combination of thiopurines and anti-TNFs compared with either medication alone (27,320,321).
Recommendations
- Vedolizumab should be used for maintenance of remission of vedolizumab-induced remission of Crohn’s disease (conditional recommendation, moderate level of evidence).
- Natalizumab should be considered for maintenance of remission of natalizumab-induced remission of Crohn’s disease patients only if JC virus is negative (conditional recommendation, moderate level of evidence).
Natalizumab monotherapy is effective for the maintenance of natalizumab-induced remission of CD (322,323). Natalizumab 300 mg every 4 weeks was superior to placebo in maintaining clinical response and clinical remission through week 36. Because of an increased risk of PML, all patients must be tested for the JC virus every 6 months, and should not receive natalizumab if positive (324). Natalizumab should not be used in combination with immunosuppressive therapy because of the increased risk of PML.
Vedolizumab monotherapy is effective at maintaining vedolizumab-induced response or remission (232). Vedolizumab 300 mg every 8 weeks was superior to placebo in maintaining clinical response and remission through week 54. Because of the gut-selective nature of vedolizumab, there is no central nervous system uptake, unlike natalizumab. To date, there has not been a reported case of PML with vedolizumab. Vedolizumab may be administered as monotherapy; however, because of the potential for immunogenicity and loss of response, combination with azathioprine/6 mercaptopurine or methotrexate may be considered. The risks and benefits of combination therapy should be evaluated in each individual patient.
Recommendations
- Ustekinumab should be used for maintenance of remission of ustekinumab-induced response of Crohn’s disease (conditional recommendation, moderate level of evidence).
Subcutaneous ustekinumab monotherapy has been shown to be effective for maintaining clinical remission among those moderate-to-severe CD patients who had demonstrated clinical response to an intravenous induction dose of ustekinumab, and this held true for those who had failed conventional therapy and those who had failed anti-TNF therapy (233).
POSTOPERATIVE CROHN’S DISEASE: MAINTENANCE, PREVENTION, AND TREATMENT
Prophylactic treatment is recommended after small intestinal resection in patients with risk factors for recurrence (Summary Statement).
Recommendations
- All patients who have Crohn’s disease should quit smoking (conditional recommendation, very low level of evidence).
Several risk factors have been identified that increase the likelihood of postoperative CD recurrence (325). The three factors that portend the greatest risk for postoperative recurrence are: (i) active tobacco smoking after surgery, especially in women and heavy smokers; (ii) patients with penetrating disease (i.e., fistulas, abscesses, and intestinal perforation); and (iii) those with two or more prior surgeries. Patients who have these risk factors should receive postoperative CD medication in an attempt to prevent future recurrence (326). Although not formally studied, those patients who progress to surgery despite treatment with an immunomodulator or biologic agent probably represent a uniquely aggressive CD phenotype and are at a high risk of postoperative recurrence. Other risk factors for postoperative recurrence include: a shorter duration between the time of diagnosis and surgery (<10 years), disease location in the ileum and colon (rather than ileum alone), perianal fistula, more severe disease leading to surgery, a longer segment of bowel requiring resection, and the need for corticosteroids before surgery. The only modifiable risk factor for postoperative CD recurrence is cigarette smoking, and all patients should be strongly encouraged to quit (327).
Recommendations
- Mesalamine is of limited benefit in preventing postoperative Crohn’s disease, but in addition to no treatment is an option for patients with an isolated ileal resection and no risk factors for recurrence (conditional recommendation, moderate level of evidence).
Mesalamine is a safe but minimally effective medication to prevent postoperative CD recurrence (328,329,330,331,332,333). A Cochrane analysis found that mesalamine reduced clinical recurrence (RR, 0.76; 95% CI, 0.62–0.94) and severe endoscopic recurrence (RR, 0.50; 95% CI, 0.29–0.84) compared with placebo, but with a NNT of 12 and 8, respectively (329,334). A subsequent systematic review and meta-analysis concluded that mesalamine is of only modest benefit in preventing postoperative recurrence compared with placebo (335). The meta-analysis included 11 randomized controlled trials with a total of 1,282 patients, and found that 5-ASAs reduced relapse compared with placebo (RR, 0.86; 95% CI, 0.74–0.99), but with a NNT of 13. The 5-ASAs were also analyzed separately as sulfasalazine and mesalamine. Sulfasalazine did not prevent relapse compared with placebo (RR, 0.97; 95% CI, 0.72–1.31) and mesalamine prevented relapse compared with placebo or no treatment (RR, 0.80; 95% CI, 0.70–0.92) but with a NNT of 10. Overall, mesalamine should only be considered if immunosuppressive therapy is not warranted or is contraindicated.
Recommendations
- Imidazole antibiotics (metronidazole and ornidazole) at doses between 1 and 2 g/day can be used after small intestinal resection in Crohn’s disease patients to prevent recurrence (conditional recommendation, low level of evidence).
Metronidazole (20 mg/kg) may significantly reduce the incidence of severe (i3-4) (Supplementary Information online) endoscopic recurrent disease compared with placebo-treated patients at 3 months after surgery and clinical recurrence at 1 year (336). Ornidazole (1 g/day) also decreases postoperative clinical recurrence at 1 year (337). However, the benefit from metronidazole and ornidazole in preventing CD recurrence is lost when these medications are stopped. In placebo-controlled trials, nearly 50% of patients were intolerant to the antibiotics, and this postoperative prevention strategy is not sustainable for most patients. Combining metronidazole (1 g/day) for 3 months with azathioprine (100–150 mg/day) for 12 months reduces endoscopic recurrent disease (i2-4) at 1 year after surgery compared with those patients just receiving metronidazole (338).
Recommendations
- Thiopurines may be used to prevent clinical and endoscopic recurrence and are more effective than mesalamine or placebo. However, they are not effective at preventing severe endoscopic recurrence (strong recommendation, moderate level of evidence).
Thiopurines have been extensively studied for the prevention of postoperative CD with some trials showing benefit and others not (338,339,340,341,342). Subsequently, there have been one Cochrane analysis and two meta-analyses. In the Cochrane analysis, thiopurines were found to significantly reduce clinical recurrence (RR, 0.59; 95% CI, 0.38–0.92; NNT=7) and severe endoscopic recurrence (RR, 0.64; 95 CI, 0.44–0.92; NNT=4) compared with placebo and was found to be superior to mesalamine (334). Similar findings were reported in a concurrent meta-analysis of four controlled trials, in which thiopurines were determined to be more effective than placebo for preventing clinical recurrence at 1 year (mean difference, 8%; 95% CI, 1–15%; P=0.021; NNT=13) and 2 years (mean difference, 13%; 95% CI, 2–24%; P=0.018; NNT=8) after surgery, and endoscopic recurrence (i2-4) (mean difference, 23%; 95% CI, 9–37%; P=0.0016; NNT=4) at 1 year after surgery (343). In another meta-analysis of five controlled trials, thiopurines were determined to be no more effective than placebo or mesalamine (controls) for preventing clinical recurrence (year 1 RR, 0.88; 95% CI, 0.60–1.30; P=0.53 and year 2 RR, 0.76; 95% CI, 0.55–1.05; P=0.10), but were more effective at preventing endoscopic recurrence (year 1 RR, 0.71; 95% CI, 0.53–0.94; P=0.02) (344). There were significantly more adverse events leading to drug withdrawal in patients receiving thiopurines compared with controls (RR, 2.57; 95% CI, 1.47–4.51; P =0.001).
Recommendations
- In high-risk patients, anti-TNF agents should be started within 4 weeks of surgery in order to prevent postoperative Crohn’s disease recurrence (conditional recommendation, low level of evidence).
- Although data are lacking in postoperative Crohn’s disease, anti-TNF therapy should be combined with an immunomodulator to decrease immunogenicity and decrease loss of response (conditional recommendation, very low level of evidence).
Growing evidence demonstrates that anti-TNF therapy is the most effective treatment to prevent postoperative recurrence and may have the potential to change the natural course of CD after surgery. There have been multiple open-label studies of adalimumab and infliximab, one small single-center randomized controlled trial of infliximab, and one large international, multicenter randomized controlled trial of infliximab (345,346,347,348,349,350,351,352,353,354,355,356). Two meta-analyses have included anti-TNFs for the efficacy of preventing postoperative CD (357,358). One meta-analysis only included one anti-TNF study, but concluded that infliximab was superior to placebo in preventing clinical and endoscopic recurrence after surgery for CD (358). In a network meta-analysis of 21 controlled trials across 5-ASAs, antibiotic, and immunomodulator treatments, anti-TNF monotherapy reduced the risk of clinical relapse (RR, 0.04; 95% CI, 0.00–0.14) and endoscopic relapse (RR, 0.01; 95% CI, 0.00–0.05) compared with placebo (357). Anti-TNF monotherapy was the most effective medication intervention for preventing postoperative CD recurrence, with large effect sizes relative to all other medication strategies (clinical relapse RR, 0.02–0.20; endoscopic relapse RR, 0.005–0.04).
Accordingly, the authors recommend anti-TNF therapy as first-line prophylactic therapy for patients at high risk for postoperative recurrence or for patients who have tried and failed or are intolerant of thiopurines. Whether combination thiopurine with an anti-TNF is more effective than monotherapy anti-TNF is not known and the postoperative trials to date have only evaluated monotherapy. CD patients treated with combination infliximab and azathioprine have higher response and remission rates compared with either medication alone (215,221). The authors suggest combination therapy but acknowledge that monotherapy anti-TNF is an acceptable postoperative treatment approach.
Risk factors for postoperative Crohn’s disease recurrence should be taken into account when deciding on treatment (Summary Statement).
Patients at low risk for postoperative CD recurrence are nonsmokers, do not have penetrating disease, and have never had a prior surgical resection. No treatment after surgery in this population with subsequently performing a 6-month postoperative colonoscopy to assess for the presence of CD recurrence would be reasonable. Patients who are nonsmokers, who have penetrating disease without a prior history of surgical resection, and who have received no prior medication should receive thiopurines with or without metronidazole, and subsequently undergo a colonoscopy at 6 months. If there is evidence of CD on the colonoscopy, then anti-TNF therapy should be added (359,360). Patients who have had a prior resection within a 10-year period should receive postoperative anti-TNF therapy with or without an immunomodulator and undergo a subsequent colonoscopy at 6 months postoperatively.
When to refer to surgery
Surgery is required to treat enteric complications of Crohn’s disease (Summary Statement).
A resection of a segment of diseased intestine is the most common surgery for a Crohn’s disease (Summary Statement).
Surgery is required in CD patients with intractable hemorrhage, perforation, persisting or recurrent obstruction, abscess, dysplasia or cancer, or medically refractory disease (361). The most common indication for a surgical resection of the intestine in CD is because of a small bowel obstruction from a fibrostenotic stricture (362). The second most common indication for bowel resection is related to penetrating CD (e.g., an internal fistula or sinus tract resulting in an abscess or phlegmon). Although an intestinal resection is the most definitive treatment for a stricture, a stricturoplasty is an option as a bowel-preserving measure in patients at risk for short gut syndrome. The management of CD requires a multidisciplinary approach between the gastroenterologist and surgeon (363). Surgery is not considered to be a failure of medication, and an early surgical consultation is appropriate in CD patients with strictures or penetrating complications.
Is surgery always required for intra-abdominal abscess?
Recommendations.
- An intra-abdominal abscess should be treated with antibiotics and a drainage procedure, either radiographically or surgically (conditional recommendation, low level of evidence).
Crohn’s disease patients who develop an abdominal abscess should undergo a surgical resection. However, some may respond to medical therapy after radiologically guided drainage (Summary Statement).
The presence of active luminal CD with a concomitant abdominal abscess is usually the result of a sinus tract or fistula, often associated with the presence of an intestinal stricture (364). Small interloop abscesses may not be amenable to percutaneous drainage; however, most CD abscesses are accessible to ultrasonographic or computed tomography-guided drainage procedures (365,366,367). Once the abscess has been drained, most patients benefit from a delayed surgical resection (368). The rationale for delaying intestinal resection until the abscess is drained is because of the fact that patients with peritonitis and intra-abdominal sepsis require a diverting, temporary ostomy before a surgical anastomosis is created. Some patients may benefit from a combination of abscess drainage followed by CD medical treatment, especially those with a new diagnosis and absence of stricturing disease (253,369). To date, there are no studies comparing percutaneous drainage followed by delayed intestinal resection vs. medical therapy.
FUTURE DIRECTIVES
Despite the recent advances in the treatment of patients with CD, there still remains a large group of patients who do not respond adequately to our current medication armamentarium. We cannot selectively determine whether an individual will respond to a particular biologic, it is more of a “wait and see” approach. We are now entering an era of precision medicine and have begun to explore factors that predict response or nonresponse. In the future, biological therapies for IBD are likely to be used more selectively based on an individual patient’s specific benefit/risk assessment, as determined by specific tissue signatures and reliable biomarkers, and will probably be adjusted throughout the course of their treatment. We will certainly expand our medical treatment war chest and uncover effective biologics with different mechanisms of action to treat our patients. If the initial biologic drug fails, patients will be able to switch to another agent and even combination biologics may become a reality.
NOVEL AGENTS
There are currently numerous novel agents in various phases of development being investigated for their ability to effectively treat patients with CD. There is an unmet need for the treatment of patients with CD. Approximately one-third of patients who are anti-TNF naive have a primary nonresponse to anti-TNF therapy. Among patients who are initial anti-TNF therapy responders, approximately one-third subsequently lose their response to therapy or become intolerant to therapy (secondary nonresponders). These secondary nonresponders can either escalate dose of their current medication, switch to another anti-TNF agent, or switch out of class (to an anti-integrin (natalizumab or vedolizumab), anti-IL-12 / 23 (ustekinumab), or to a novel mechanism. Those individuals who switch to therapy within class have less benefit than individuals who are TNF naive.
Some of the other agents under different stages of development for the treatment of patients with CD include other anti-integrins such as etrolizumab (which is a dual action anti-integrin that inhibits both α4β7 and αEβ7) or ozanimod (a potent sphingosine-1-phosphate receptor modulator that inhibits the egress of lymphocytes from lymph nodes) (370,371). Several other agents in early phases of development include the anti-IL-23 agents, risankizumab (372) and brazikumab (373), and the selective Janus kinase-1 inhibitors, filgotinib (374) and upadacitinib (formerly ABT-494) (375).
CONFLICT OF INTEREST
Guarantor of the article: Gary R. Lichtenstein, MD, FACG.
Specific author contributions: Gary R. Lichtenstein, Edward V. Loftus, Jr, Kim L. Isaacs, Miguel D. Regueiro, Lauren B. Gerson, and Bruce E. Sands: planning the paper, collecting and interpreting data, and drafting the manuscript. Approved the final draft submitted. Lauren B. Gerson performed the Grade analysis. She did not approve the final draft submitted as she passed away before approval.
Financial support: The American College of Gastroenterology supported creation of this guideline.
Potential competing interests: Dr. Lichtenstein has served as a consultant or received funds for CME programs from AbbVie, Actavis, Alaven, CellCeutrix, Celgene, Ferring, Gilead, Hospira, Janssen Orthobiotech, Ironwood, Luitpold/American Regent, Merck, Pfizer, Prometheus Laboratories, Romark, Salix Pharmaceuticals/Valeant, Santarus/Receptos/Celgene, Shire Pharmaceuticals, Takeda, UCB. He has received research funding from Celgene, Janssen Orthobiotech, Takeda, Salix Pharmaceuticals/Valeant Pharmaceuticals, Santarus/Receptos/Celgene, Shire Pharmaceuticals. He has served as an editor and received honorarium for Gastro-Hep Communications, McMahon Publishing, Springer Science, and Business Media and Up-To-Date. He has received book royalty from SLACK. He has received support for IBD fellowship training from: Janssen Orthobiotech, Takeda, and Pfizer. Dr. Loftus has received research support from Janssen, Takeda, UCB, AbbVie, Pfizer, Amgen, Genentech, Receptos, Gilead, Celgene, Seres Therapeutics, MedImmune, Allergan, and Robarts Clinical Trials. He has consulted for Janssen, Takeda, UCB, AbbVie, Pfizer, Amgen, Eli Lilly, Celgene, Celltrion Healthcare, and Napo Pharmaceuticals. Dr. Sands has been a consultant and received research grants from Pfizer, AbbVie, Amgen, AstraZeneca, Celgene, Janssen, MedImmune, Prometheus Laboratories, and Takeda, has been a consultant for Akros Pharma, Allergan, Arena Pharmaceuticals, Forest Research Institute, Boehringer-Ingelheim, Forward Pharma, Immune Pharmaceuticals, Lilly, Luitpold Pharmaceuticals, Receptos, Salix Pharmaceuticals, Syngergy Pharmaceuticals, Theravance Biopharma R&D, TiGenix, TopiVert Pharma, UCB, and Vedanta Biosciences, and has received honoraria for speaking in a CME program from the American College of Gastroenterology. Dr. Regueiro has received research support from Janssen, Abbvie, and Takeda, and has served as a consultant and was on advisory boards for Amgen, AbbVie, Janssen, Takeda, Pfizer, UCB, Celgene, and Miraca. Dr. Isaacs has received research support from Janssen, Takeda, UCB, Abbvie, Roche, Eli Lily, and Celgene. She has received support for IBD fellowship training from Takeda, Abbvie, and Pfizer. She is part of DSMB for Medimmune and Janssen. Dr. Gerson declares no conflict of interest.
REFERENCES





Discover more from reviewer4you.com
Subscribe to get the latest posts to your email.