ACG Clinical Guideline: Alcohol-Associated Liver Disease : Official journal of the American College of Gastroenterology

INTRODUCTION
Alcohol-associated liver disease (ALD) is a leading cause of preventable liver-related morbidity and mortality worldwide, including the United States. Harmful drinking (≥3 drinks/d or ≥21/wk in men and ≥2 drinks/d or ≥14/wk in women) is a risk factor for liver damage and ALD and often occurs in the setting of alcohol use disorder (AUD) (1,2). This pattern of alcohol use is associated with negative social and/or health consequences. The spectrum of ALD ranges from steatosis and steatohepatitis to progressive fibrosis, cirrhosis, and hepatocellular carcinoma (HCC) and includes the unique presentation of alcohol-associated hepatitis (AH), with development of acute on chronic liver failure (ACLF) in more severe forms (Figure 1). The diagnosis of ALD requires identification of chronic, harmful alcohol use, by patient report or detection of alcohol biomarkers, and exclusion of other diseases affecting the liver. It should be acknowledged that harmful alcohol use can accelerate progression of other hepatic diseases including metabolic dysfunction-associated steatotic liver disease (MASLD). Individuals with early ALD may be asymptomatic, with steatosis or steatohepatitis and early stage fibrosis. Advanced patients with ALD may have advanced fibrosis including cirrhosis, complications of cirrhosis with decompensating events (ascites, hepatic encephalopathy, variceal bleeding, and HCC), or symptomatic AH with jaundice and/or ACLF (1). Treatment of AUD with achievement of sustained abstinence is the most effective strategy to prevent disease progression and improve long-term outcomes at any stage of ALD. Liver transplantation (LT) remains a definitive treatment option for patients with end-stage liver disease due to alcohol-associated cirrhosis and/or HCC.

Disease spectrum of alcohol-associated liver disease. HCC, hepatocellular carcinoma.
Important advances in our understanding of ALD have occurred, including (i) insights into the natural history and prevalence of early ALD among at-risk individuals with harmful alcohol use or AUD; (ii) increasing prevalence of severe forms of ALD in younger individuals, women, and minorities such as Hispanics and American Indians; (iii) genetic and environmental factors that influence disease susceptibility and progression; (iv) noninvasive techniques to assess liver fibrosis in patients with early ALD; (v) identifying patients at high risk of disease progression; (vi) clinical criteria for diagnosis of AH simplifying decisions on treatment and recruitment in clinical trials; (vii) benefits of early liver transplantation (LT) (i.e., with <6 months of alcohol abstinence) with increasing momentum on acceptability and refinement of selection criteria for this salvage therapeutic option in patients with severe AH; and (viii) the role of multidisciplinary integrated clinical care models including hepatology and addiction specialists to manage the dual pathologies of liver disease and of AUD, respectively, to improve long-term outcomes of patients with ALD. Although significant progress has been made in the therapeutic pipeline for patients with ALD and AH, continued efforts are critical in the development of effective pharmacotherapeutic options.
The authors were invited by the Board of Trustees and Practice Parameters Committee of the American College of Gastroenterology (ACG) to develop this practice guideline document on the management of patients with ALD. Recommendations based on patient-intervention-comparison-outcome (PICO) format/Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) analysis are summarized in Table 1. These recommendations and guidelines should be tailored to individual patients and circumstances in routine clinical practice. Key concepts and recommendations based on author expert opinion and review of literature are summarized in Table 2.

Recommendations

Key concepts and statements
To develop these guidelines, a search was performed on the Ovid search platform: Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R), EBM Reviews Cochrane Central Registry of Controlled Trials, EMBASE, and PsycInfo for the period January 1980 to December 2022. Where appropriate, the PICO method was used as a means of addressing key clinical questions specific to patients with ALD. When a PICO format was not appropriate, the area of interest was included as a statement or key concept. To evaluate the level of evidence and strength of recommendations, we used the GRADE system, as suggested by the ACG Practice Parameters Committee. The strength of recommendation is graded as strong or conditional as a consensus among the authors, considering the weight of desirable and undesirable effects of intervention. The level of evidence was determined by members of the GRADE team at ACG (R.J.W. and B.G.S.), and this determination was made independently of the other authors, and designated as high, moderate, low, and very low, considering the confidence in the effect estimate based on current literature.
EPIDEMIOLOGY AND DISEASE BURDEN
Key concept/statement
ALD is one of the main causes of chronic liver disease worldwide and is the leading cause of liver-related mortality in the United States (3). Globally, there are 3 million deaths annually attributed to harmful alcohol use, accounting for 5.3% of all deaths and 13.5% of deaths in people aged 20–39 years (4). According to the National Institute of Alcoholism and Alcohol Abuse (NIAAA) Surveillance Report on mortality in 2019, cirrhosis was the 11th leading cause of death in the United States, with about half of cirrhosis-related deaths due to alcohol (5). The crude death rate from cirrhosis of any etiology was 14.6 deaths per 100,000 persons, whereas the rate from alcohol-associated cirrhosis was 7.3 per 100,000 (5). There has been a continued narrowing of the gender gap, with increasing numbers of women with ALD. The World Health Organization has established a future goal of reducing the death rate from cirrhosis to below 8.2 deaths per 100,000 population (3).
Key concepts/statements
Alcohol contributes to approximately 48% of cirrhosis-related hospitalizations and more than 40% of listings for LT in the United States (7–10). The LT activity increased by >50% for AH with a 4-fold increase between 2003 and 2018 among those aged younger than 40 years (7,8). An increase in LT for ALD has been evident since 2014, reflecting a decreased LT need for hepatitis C virus (HCV) because of availability of direct-acting antivirals, a true increase in the incidence of ALD, and wider acceptance of LT for severe AH (11). The COVID-19 pandemic further increased the healthcare burden of ALD secondary to a 14% rise in alcohol use over prior years, resulting in increased ALD mortality and ALD-related transplant listing during and after the pandemic (8,12,13). Overall, AUD-related mortality rates increased during the pandemic by 24.8% in 2020 and 22% in 2021 compared with prepandemic rates (14). Hospitalizations for ALD have also increased especially among younger individuals, women, and minorities such as American Indians and Hispanics (9,15). Women are less likely to use AUD therapies and prevention services than men, possibly related to more perceived stigma, conflicting child/family and personal needs, and financial barriers (16). A modeling study showed that the 1-year increase in alcohol consumption during the COVID-19 pandemic could result in 8,000 additional ALD-related deaths, 18,700 cases of decompensated cirrhosis, and 1,000 new diagnoses of HCC between 2020 and 2040 (17). From 2010 to 2016, ALD had the highest economic cost burden for hospitalizations of any etiology of liver disease in the United States, with a total cost of $22.7 billion (95% confidence interval [CI] $22.1–$23.2 billion), and although hospitalizations for hepatitis B virus (HBV), HCV, MASLD, and HCC down trended or remained stable over this time, there was a near doubling of hospitalization for ALD (6). These figures become more relevant considering that ALD contributes to 50% of overall burden of liver disease but only receives 5% of the mean research funding (18).
RISK FACTORS FOR ALD
Key concepts/statements
Harmful drinking is a pattern of alcohol use leading to health or psychosocial problems and is the primary risk factor for the development of ALD (19). Increasing evidence suggests that there are minimal or even no health benefits to drinking and that any amount of alcohol use has potential to cause harm; however, it is estimated that only 10%–20% of individuals with chronic heavy alcohol use develop cirrhosis (20). There is a dose-dependent and duration-dependent relationship between the amount of alcohol intake and the likelihood of developing advanced forms of ALD (21–23), yet extensive individual variability exists because of genetic factors and the existence of comorbidities (e.g., metabolic syndrome). Furthermore, patients with early ALD are reported to consume similar amounts of alcohol to those with AH, suggesting that there are other factors (Figure 1) which contribute to the risk for and severity of ALD (24). Those factors may include sex and drinking outside of meals. For example, in the Million Women UK Study, among women who drank, drinking with meals carried a 31% lower relative risk for cirrhosis when compared with usually drinking outside of meals (23). Women are at a higher risk for ALD at a lower daily intake of alcohol compared with men, probably due to higher body fat component and lower gastric alcohol dehydrogenase activity (25). Binge drinking (see Table 3 for this and other definitions of alcohol use patterns) is reported in 26% of individuals aged 18 years or older in the United States (19). It is speculated that higher blood alcohol levels with binge and high intensity drinking promote bacterial translocation (26) and liver fibrosis (27); however, the exact role of binge drinking as a risk factor for cirrhosis remains to be established (28). Although daily drinking is associated with higher risk of cirrhosis (29), it is plausible that heavy drinking with superimposed binge and high intensity drinking have additive effects. Importantly, binge drinking in patients with underlying metabolic syndrome has been associated with higher likelihood of cirrhosis (30).

Definitions of alcohol drink and patterns of alcohol use
Key concept/statement
Large epidemiological studies have suggested that wine or beer consumption, perhaps due to antioxidant properties, is less associated with ALD than liquor-based drinking (31,32). However, a study of 43,242 men conscribed to military service in Sweden in 1970 with follow-up data obtained from population-based registries showed only a trend toward reduced risk for severe liver disease in men consuming more than 50% of alcohol as wine compared with those consuming <1% of alcohol as wine (hazard ratio [HR] 0.70, 95% CI 0.48–01.02, P = 0.06) (33). Studies are needed to examine the effects of specific alcohol additives and adulterants on the likelihood or severity of ALD.
Key concept/statement
Earlier studies have shown that monozygotic twins have a higher concordance for alcohol-associated cirrhosis than dizygotic twins (34). Significant variant alleles conveying risk for the development and severity of ALD include the patatin-like phospholipase domain containing protein 3 (PNPLA3) rs738409, transmembrane 6 superfamily member 2 (TM6SF2), and membrane bound O-acyltransferase domain containing 7 (MBOAT7) rs641738 (35,36). Interestingly, the combination of polymorphisms of some of these genes in the presence of diabetes predicts the development of cirrhosis (37). Variations in PNPLA3 also predispose to the development of HCC in patients with alcohol-associated cirrhosis (36,38). In another study, the Pi*Z homozygous variant of α-1 antitrypsin gene in individuals with AUD was more frequently present in those with cirrhosis compared with those without cirrhosis (6.2% vs 2.2%, P < 0.001), with a 5.8-fold (95% CI 2.9–11.7)-adjusted risk for cirrhosis, whereas the Pi*S homozygous variant only trended toward risk of cirrhosis with an adjusted odds ratio of 1.47 (95% CI 0.99–2.19) (39). It should be acknowledged that these genetic association studies are mostly performed in White and/or Asian populations, with very little representation of Black, Native American, and Hispanic populations. Less is known about the genetic determinants of AH; however, the PNPLA3 rs738409 variant has shown an association with its development (40) and mortality (41). Thus, larger studies of this allele are warranted in patients with AH.
Recommendation
In a large study of 128,934 individuals receiving health examination between 1978 and 1985, smoking ≥20 cigarettes daily was independently associated with a 3-fold risk of ALD cirrhosis (42). In a more recent study, smoking >10 g of tobacco per day (>16 cigarettes) was associated with 1.6-fold risk of developing ALD cirrhosis, with the effect more significant in women than men (95% CI 1.6–9.4 vs 0.9–3) (43). Furthermore, the Million Women Study of >1.2 million women in the United Kingdom showed that the risk of cirrhosis was higher with current smoking and drinking >7 drinks a week (RR 8.02, CI 6.84–9.4) than being a never smoker with the same level of drinking (RR 2.09, CI 1.72–2.53) (44). In addition, multiple epidemiologic studies have found concurrent tobacco and heavy alcohol use to increase the risk of HCC (45–47). Although, based on animal studies, multiple toxins (nitrosamines, aromatic hydrocarbons, and other alkaloids) in cigarette smoke have been shown to cause systemic inflammation, oxidative stress, tissue hypoxia, and generation of free radicals, all of which may promote hepatic fibrosis, further animal studies have found that nicotine independently promotes liver fibrosis (48,49).
Recommendations
Obesity and metabolic syndrome increase the risk of advanced liver disease in heavy drinkers (50). Epidemiologic studies show that a body mass index of >30 k/m2 in patients with >3 drinks per day increases the risk of liver disease including elevated transaminases, steatosis, severity of fibrosis, cirrhosis, and HCC (51). Moreover, the presence of obesity among heavy drinkers is associated with increased likelihood of having cirrhosis (50,51). In another study, individuals with harmful alcohol consumption who are obese or overweight compared with normal weight were at 1.5-fold risk for any liver disease and 2.2-fold risk for death (52). Although large epidemiological studies initially suggested that moderate alcohol consumption may protect against MASLD (53,54), more recent studies using individual data indicate that even moderate drinking can favor the development of liver disease in people with obesity and metabolic syndrome (55,56).
Diabetes also seems to exacerbate the development of liver disease in people who drink. A recent study revealed that having diabetes in the setting of heavy alcohol use was associated with a 6-fold higher risk of a liver-related admission, mortality, and HCC (57). Interestingly, although bariatric surgery can alleviate or reverse MASLD, it can be a risk factor for the development of AUD and consequent ALD (58,59). Gastric bypass anatomy is associated with a 2- to 3-fold increased risk for the diagnosis of AH (60). Furthermore, a recent study of the national inpatient sample showed that among admissions for alcohol-associated cirrhosis (N = 10,168), a concurrent diagnosis of AH was higher in those with vs without a history of Roux-en-Y gastric bypass (18.8% vs 17% P = 0.032) (61).
Recommendation
Alcohol use is a frequent cofactor in individuals with HCV infection, and heavy daily alcohol use (>50 g) was shown to be an independent risk factor for hepatic fibrosis progression in HCV patients with viremia (62). The dose-dependent deleterious effects of alcohol in HCV have been recently revealed in a meta-analysis of 33 studies from 21,919 participants, demonstrating that each daily drink increased the risk for cirrhosis, decompensated cirrhosis, and liver-related mortality by 11.2% (63). Moreover, individuals with chronic HCV who drank > 6 standard drinks daily had a >50-fold increased risk of developing HCC than those who did not drink (64).
Recommendation
Several studies have shown that alcohol drinking worsens the course of HBV liver disease. In a cohort study of adults hospitalized with chronic liver disease and concurrent alcohol use of > 3 drinks per day, HBsAg-positive patients had 2-fold increased odds of cirrhosis compared with patients without HBV (odds ratio [OR] 4.8, CI 1.8–12.4 vs OR 2.4, CI 1.3–4.2) (65). In a prospective cohort study of 966 patients with cirrhosis (2000–2009) and followed until 2011, the annual incidence of HCC was 9.9% in 132 patients with HBV infection and AUD, 4.1% in patients with HBV infection who did not use alcohol, and 2.1% in patients with AUD without HBV infection. The 10-year cumulative incidence of HCC was 52.8% vs 39.8% vs 25.6% (P < 0.001) for the 3 respective groups (66). For patients with cirrhosis and HBV infection with AUD, higher HBV DNA levels were associated with risk of HCC, while treatment with oral antiviral drugs for HBV infection protected against HCC development (66). Furthermore, in another prospective cohort study of 1,515 patients with cirrhosis, those with HBV and heavy chronic alcohol use (>80 g of alcohol daily for > 5 years) had a higher incidence of HCC occurring over a 10-year follow-up compared with patients with HBV cirrhosis without heavy alcohol use (crude HR 2.13, 95% CI 1.62–2.81, P < 0.001) (67).
DIAGNOSIS AND TREATMENT OF AUD
Recommendation
Key concept/statement
Due to various susceptibility factors, individuals with long-term harmful alcohol use are at risk for AH, cirrhosis, and HCC (68). Patients with ALD often present at an advanced stage of liver disease and progress faster to advanced disease and/or complications compared with other liver diseases including MASLD and HCV (69,70). Many patients with ALD present for medical care after they have developed complications of cirrhosis (71), with previous healthcare encounters representing missed opportunities for identifying individuals with harmful alcohol use and achieving the downstream benefits of preventing ALD and its complications (72–74). The ideal screening tool and setting for identifying individuals with AUD should be tailored to individual populations given global healthcare and technology disparities (75). The AUD Identification Test (AUDIT), a 10-item patient self-reported questionnaire, is an accurate and validated tool for screening individuals for AUD and grading its severity. A shorter version, Alcohol Use Disorders Identification Test-Consumption, composed of 3 questions, is quick to use in clinical practice, with similar accuracy to the full AUDIT tool (76). The AUDIT score demonstrated a linear relationship with mortality in a meta-analysis of 7 studies on 309,991 persons. In this study where 18,920 deaths were observed over 2–10 years of follow-up (72), those with AUD had a 24% higher relative risk of dying compared with moderate drinkers (72). A limitation of this meta-analysis was that 97% of study population represented veterans, with a sparse representation of young adults and women. The cutting down annoyance by criticism guilt eye opener questionnaire, another tool to gauge alcohol use, assesses the dependence on alcohol and does not quantify alcohol use. A single question “how many times in the past year have you had 5 or more drinks (4 or more for women) at one time” can also be used to identify those with harmful alcohol use.
Universal screening for AUD at any healthcare encounter
Screening all patients for AUD is feasible in the healthcare setting (77–80). For example, admitting nurses in a large hospital emergency department performed alcohol use screening in 637 patients using AUDIT and modified-for-Australia version of the Paddington Alcohol test. The Australia version of the Paddington Alcohol test performed moderately well compared with AUDIT (kappa statistics of 0.63, P < 0.001), with a sensitivity and specificity of 72.5 (65.3%–79.7%) and 90.8 (88.3%–93.4%), respectively (81). A targeted approach to screening in the healthcare setting by selecting individuals with complaints anecdotally associated with harmful drinking has also been explored. A multicenter study of 3,021 patients from 29 primary care offices found that alcohol screening in a population of individuals with mental health conditions, gastrointestinal conditions, hypertension, and minor injuries had a higher odds ratio for harmful alcohol consumption than in a universally screened population without these complaints (1.65, 95% CI 1.41–1.93) (82).
Key concept/statement
Indirect biomarkers of alcohol reflecting alcohol-induced tissue damage (i.e., gamma-glutamyltransferase, mean corpuscular volume, and carbohydrate-deficient transferrin) (83) have high individual variability and limited utility (34). Direct alcohol biomarkers including blood alcohol concentration (84), ethyl glucuronide, ethyl sulfate (85–91), and phosphatidylethanol (92) seem to have better performance than indirect biomarkers. For the detection of recent alcohol use in individuals with liver disease (93), alcohol biomarkers have variable temporal windows of detection, sensitivity, and specificity as detailed in Table 4. For patients who disclose heavy recent drinking, alcohol biomarkers provide no added clinical utility. Biomarkers may be helpful to identify recent alcohol use in patients who cannot be interviewed because of encephalopathy or intoxication or when reported alcohol use is suspected to be inaccurate.

Biomarkers of alcohol use
Recommendation
Nonpharmacologic therapies for AUD include motivational interviewing, screening, brief intervention (BI), referral, and treatment, BI, cognitive behavioral therapy, motivational enhancement therapy, and 12-step facilitation/Alcoholics Anonymous. The former 3 approaches can be performed by any healthcare provider using a foundation of motivational interviewing techniques, while the latter 3 require specialty expertise. Motivational interviewing is a nonjudgmental, nonconfrontational conversational technique aimed to increase a person’s awareness of the problems caused, consequences experienced, and risks faced because of an undesirable behavior (https://store.samhsa.gov/sites/default/files/SAMHSA_Digital_Download/PEP20-02-02-014.pdf). It is important that the interviewer exhibits an empathic attitude and a collaborative approach, regarding the individual’s autonomy (94,95). Screening, BI, referral, and treatment is a comprehensive approach with proven efficacy in reducing short-term and long-term (96,97) alcohol use in persons with AUD. BI based on the 5 “A” model (ask about use, advice to quit or reduce, assess willingness, assist to quit or reduce, and arrange follow-up), where physician feedback on alcohol-related harms was shown to reduce alcohol use in a study of more than 9,000 individuals with mild AUD (AUDIT score 8–20) in a primary care setting (77). Seven patients needed to be treated to achieve reduction of alcohol use to within recommended limits in one patient (77). A 2018 meta-analysis of 69 studies including more than 33,000 participants showed a reduction in alcohol consumption by 20 g/wk after a BI in the primary care setting (98). A 2018 Cochrane review showed that 12-step facilitation/Alcoholics Anonymous had the most promise for decreasing drinking behavior when compared with cognitive behavioral therapy or no treatment; however, liver-related endpoints were not reported (99).
Recommendations
Pharmacotherapy of AUD is effective (1,100) and is associated with reduced risk of ALD and disease progression in those with cirrhosis (101,102). In the setting of ALD cirrhosis, the use of medication-assisted therapies is cost-effective because of benefits in reducing clinical decompensation and readmission to the hospital (103). There are 3 US Food and Drug Administration (FDA)-approved medications (disulfiram, acamprosate, and naltrexone) for AUD and others that have shown utility in patients that are not US FDA-approved. In patients with advanced liver disease including cirrhosis and AH, baclofen (GABA-B receptor agonist), a non-US FDA-approved drug, has been studied the most. Baclofen use for an average duration of 5.8 months has been shown to safely reduce alcohol use in patients with AH (104) and increase abstinence rates in those with ALD cirrhosis (105,106). The medication is started in a dose of 5 mg 3 times a day, with dose escalation at 3–5-day intervals based on patient tolerance to a maximum dose of 15 mg 3 times a day.
Acamprosate does not undergo hepatic metabolism, and a recent retrospective analysis suggests that its use in cirrhotic patients is safe (107); however, a retrospective cohort study revealed that acamprosate use for the treatment of AUD in individuals without a diagnosis of ALD at the start of treatment was associated with the development of ALD (OR 2.59, 95% CI 1.84–3.61, P < 0.001). However, this could have been a selection bias with preferential treatment of those at risk for development of ALD, or it is possible that the diagnosis of ALD was missed before recruiting patients into the trial. Nevertheless, acamprosate use for AUD trended to a higher odds ratio for the development of hepatic decompensation in individuals with well-compensated cirrhosis at the start of treatment (OR 1.99, 95% CI 0.99–4.059, P = 0.06) (102). If acamprosate is used, caution should be taken in patients with concurrent kidney disease, with dose adjustment if the creatinine clearance is between 30 and 50 and avoidance if below 30 mL/min. Both short-term and long-term acting forms of naltrexone may be used in individuals with early ALD and in those with compensated cirrhosis but should be avoided in patients with decompensated cirrhosis or liver failure and used cautiously in patients with kidney disease (108). There are no data for acamprosate or naltrexone on the duration of treatment and use in patients with AH.
Other pharmacological agents with off-label use for AUD include gabapentin and topiramate (109). Gabapentin and topiramate have demonstrated acceptable safety profiles in individuals with ALD (102), although large, prospective trials are needed. Data are emerging on the potential role for glucagon like peptide-1 receptor agonists in the treatment of AUD (110).
Despite having US FDA approval for AUD, disulfiram is contraindicated in individuals with liver disease of any spectrum because it is completely metabolized by the liver and hepatotoxic. Idiosyncratic liver injury of an immunoallergic mechanism has been well-described with disulfiram use and, although rare, seems more common in individuals with pre-existing liver disease (111). Furthermore, disulfiram does not seem effective in preventing development or progression of liver disease in individuals with AUD. In a retrospective cohort study of patients lacking ALD, those treated with any pharmacologic agent for AUD had a lower odds ratio for the development of ALD (OR 0.37, CI 0.31–0.43, P < 0.001); however, when disulfiram was examined in disaggregate, it showed no effect (OR 0.86, CI 0.43–1.61, P = 0.66). In individuals with cirrhosis, treatment with any pharmacologic agent for AUD was protective against hepatic decompensation (OR 0.35, CI 0.23–0.53, P < 0.001); however, when analyzed in disaggregate, disulfiram again showed no effect (OR 2.59, CI 0.54–13.26, P = 0.24) (102).
Key concept/statement
Recommendation
AWS is a common condition affecting alcohol-dependent patients who abruptly discontinue or markedly decrease alcohol consumption. A recent study showed that AWS is frequent in patients with AH and negatively affects survival (112). Mild or moderate AWS usually develops within 6–24 hours after the last drink, and symptoms may include nausea/vomiting, hypertension, tachycardia, tremors, hyperreflexia, irritability, anxiety, and headache. These symptoms may progress to more severe forms of AWS, characterized by delirium tremens, generalized seizures, coma, and even cardiac arrest and death. Older individuals are at greater risk for delirium tremens. Those with moderate or severe AWS are typically monitored in an intensive care unit, where vital signs, volume status, and neurological function can be monitored closely. Severity scores for AWS such as the Clinical Institute Withdrawal Assessment are useful in guiding management, although they have not been validated in persons with severe ALD and a symptom-triggered approach is preferred (113–117). Benzodiazepines are the most used drugs to treat AWS. Long-acting benzodiazepines (e.g., diazepam and chlordiazepoxide) protect against seizures and delirium; short-acting and intermediate-acting benzodiazepines (e.g., lorazepam and oxazepam) are safer for patients with poor liver function (118,119). Oral administration is preferred for administration of benzodiazepines and barbiturates (112). Patients with AWS and concomitant hepatic encephalopathy should be treated for both conditions. Of note, benzodiazepines may precipitate and worsen hepatic encephalopathy; thus, careful monitoring and the dose titration are critical for optimal outcomes. Given the side effects of benzodiazepines in patients with advanced liver disease and the potential for abuse with repeated use, other drugs such as baclofen, clonidine, gabapentin, and topiramate have been proposed to treat AWS in persons with ALD including alcohol-associated cirrhosis. However, the efficacy and safety of these medications in individuals with AH is unknown, and therefore, prospective studies are required.
ALD DISEASE SPECTRUM
Key concepts/statements
Fibrosis assessment among asymptomatic individuals with suspected ALD (Figure 2) is important because fibrosis correlates with long-term outcomes including survival (120–122). Liver biopsy is an invasive and costly procedure that is indicated when there are diagnostic uncertainties or suspected competing diagnoses. Several NITs have been assessed in this population (1,123). Among blood-based nonpatented markers, Fibrosis-4 (FIB-4) has been most studied and shown to have high sensitivity (80%–90%), but low specificity (60%–70%) in excluding advanced fibrosis (F3-4). The enhanced liver fibrosis score and FibroTest are patented blood-based biomarkers with higher specificity (80%–90%), but with higher cost and limited availability, especially in resource-constrained settings (120). It should be acknowledged that enhanced liver fibrosis is not as well validated in patients with ALD as other etiologies such as HCV and MASLD (124). Furthermore, platelets can be reduced by active alcohol use, which can affect the accuracy of FIB-4 as a noninvasive serological marker for fibrosis assessment in patients with ALD (1). Among radiological tests, vibration-controlled transient elastography, a test of liver stiffness measurement (LSM), has been most extensively evaluated for fibrosis assessment in patients with ALD. Multiple meta-analyses have found acceptable sensitivity and specificity, especially for advanced fibrosis (F3-F4) (122,125,126). For example, in a meta-analysis of 1,026 patients with ALD using individual patient data, a cutoff LSM of 12.1 kPa was fairly accurate to identify advanced fibrosis with receiver operating characteristics of 0.90 (95% CI 0.86–0.94) (122). It should be noted that underlying inflammation and steatohepatitis as reflected by aspartate aminotransferase levels >200 I/L and/or elevated serum bilirubin may confound and overestimate the LSM in patients with ALD (122). As the fibrosis stage is the strongest predictor of prognosis in liver disease (127), individuals with advanced fibrosis and active drinking should be referred to a liver specialist and an alcohol addiction specialist (121).

Integrated multidisciplinary care model for management of the dual pathology of alcohol use disorder and of alcohol-associated liver disease at any spectrum of liver disease. AH, alcohol-associated hepatitis; ALD, alcohol-associated liver disease; AUD, alcohol use disorder; AUDIT, AUD Identification Test; AUDIT-C, Alcohol Use Disorders Identification Test-Consumption; DSM-V, diagnostic and statistical manual.
Key concepts/statements
ALD is often undetected until irreversible, late-stage decompensated disease manifests. Consequently, there is an unmet need for effective and economically reasonable pathways to screen for advanced fibrosis among persons who drink alcohol. Studies have demonstrated that the use of NITs is cost-efficient in detecting advanced fibrosis in people with excessive alcohol intake (128,129). Furthermore, in a study compiling prospective data from 6 independent cohorts of 6,295 individuals, vibration-controlled transient elastography screening of the general population was less cost-effective than screening of individuals with heavy alcohol use with the number needed to detect 1 case of significant fibrosis (F2 or higher) being 12.5 (130). It is possible that thresholds to identify those who warrant screening are lower in patients with repeated episodes of binge drinking and those with comorbidities (131), although more data are needed. Although there are no data on the frequency of repeating screening tests, it may be reasonable to screen annually among those identified as having low risk for advanced fibrosis but who continue to use alcohol.
MANAGEMENT OF ALD
Recommendation
Patients with ALD are suffering from 2 disorders, one of liver disease and the other of AUD. To date, the most effective therapy to attenuate the clinical course of ALD and even reverse liver damage is prolonged alcohol abstinence (132,133). Increasing evidence is demonstrating that integrated care with a hepatologist and an addiction specialist is more effective than the absence of one (132,133) (Figure 2). AUD treatment in patients with ALD cirrhosis and AH associates with improvement in patient survival, decompensating events, and complications of cirrhosis, as well as reduced 30-day readmissions (101,134–136). However, it should be noted that receiving treatment for AUD, even in advanced ALD, is the exception rather than the rule. In a retrospective cohort study of more than 35,000 veterans with cirrhosis and AUD, receipt of AUD treatment in a cohort of these patients was associated with reduction in decompensation and improved patient survival within 6 months of treatment (101). Only 14% of veterans with ALD, however, received any AUD treatment, with <1% receiving pharmacotherapy. In a systematic review of 13 studies (5 of which were randomized controlled) on 1,945 patients (137), abstinence rates, however, were higher in a randomized controlled study with an integrated multidisciplinary care model with hepatologists and addiction specialists in a colocated clinic compared with usual care of AUD (74% vs 49%, P = 0.02) (138). In another meta-analysis of 6 studies on 649 LT recipients for ALD, an integrated care model compared with standard follow-up by only hepatology in a transplant clinic was associated with a lower rate of relapse to alcohol and long-term patient mortality with odds ratios of 0.56 (95% CI 0.36–0.87) and 0.29 (95% CI 0.08–0.99), respectively (139).
Key concepts/statements
HCC screening
Patients with advanced fibrosis or cirrhosis are at an increased risk of developing HCC, with an annual incidence of 2.5%–2.9% reported in 2 separate studies (140,141). In a meta-analysis of 18 studies on 148,333 patients with ALD cirrhosis, the incidence of HCC was 1%, 3%, and 9% at 1-, 3-, and 5-year follow-up, respectively. This risk was higher in patients enrolled in a surveillance program vs those not undergoing regular HCC surveillance (142). Ultrasound examination with or without α-fetoprotein estimation every 6 months is used to screen patients with ALD cirrhosis for HCC similar to any other patient with cirrhosis (143).
Hepatic encephalopathy
In patients with altered mental status, causes other than hepatic encephalopathy should be screened for when suspected, especially among individuals with clinical neuropsychiatric features which are atypical for a diagnosis of hepatic encephalopathy. For example, seizures, focal neurological deficits, severe headache, and encephalopathy refractory to all measures should point toward an alternate cause such as stroke, subdural hematoma, drug overdose, meningitis, and fungal infections of the central nervous system. A drug screen is recommended in selected individuals. Imaging of the head and cerebral spinal fluid studies may be required (144). It is also important to rule out Wernicke encephalopathy as a cause for altered mental status because it has its own prognostic and management implications (145,146), especially when considering LT for patients with ALD.
Nutrition
Every patient with ALD requires assessment of nutritional status because malnutrition is frequently present in these patients (147). Detailed clinical evaluation using the subjective global assessment tool is commonly used to assess the nutritional status (147). Nutritional goals for patients with cirrhosis from ALD are similar to those for all patients with cirrhosis with repletion of vitamin and mineral deficiencies (thiamine, vitamin B12, and zinc) common in AUD if alcohol use is recent or ongoing (148). This is covered in detail in a subsequent section under the management of AH.
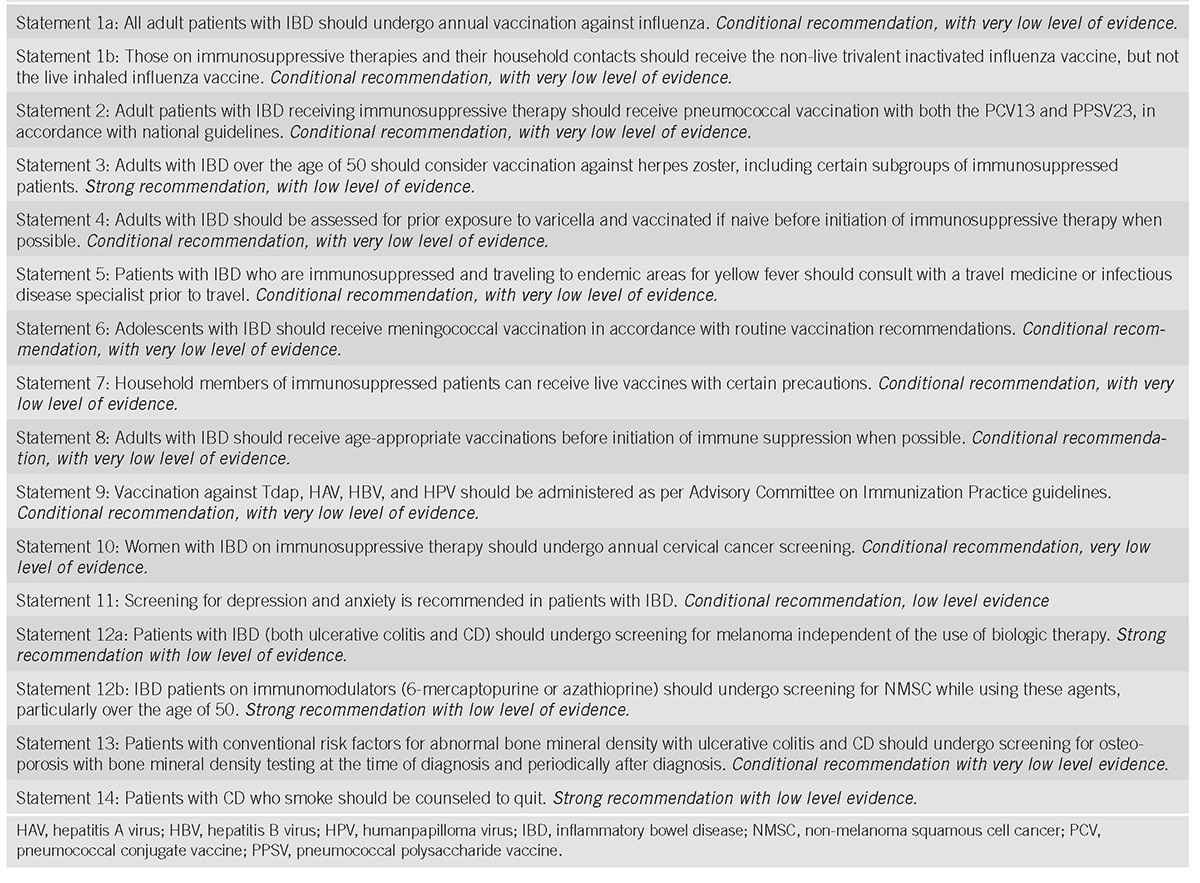
Vaccinations
Individuals with chronic liver disease should have vaccination against hepatitis A virus, HBV, influenza, pneumococcus, herpes zoster, tetanus, diphtheria, pertussis, and SARS-CoV-2 (149).
LT
Individuals with decompensated alcohol-associated cirrhosis or severe AH should be considered for referral for LT (1,150).
AH
Key concepts/statements
Among patients with suspected heavy alcohol use and new onset or worsening jaundice, clinicians should have a high suspicion for AH given its high short-term mortality. The NIAAA has proposed clinical criteria (Table 5) for the diagnosis of probable AH, which can spare severely ill patients the risk of liver biopsy. However, when the diagnosis is uncertain and 1 or more of the criteria are not met, a liver biopsy should be considered (Figure 3).

NIAAA and grading criteria of AH

Algorithmic approach toward diagnosis and management of alcohol-associated hepatitis. ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCS, budd chiari syndrome; HE, hepatic encephalopathy; HEV, hepatitis E virus; HCC, hepatocellular carcinoma; PVT, portal vein thrombosis.
Clinical features of AH include nonspecific constitutional symptoms and symptoms attributable to advanced ALD. Although evidence of hepatic decompensation is not required to make the diagnosis of AH, physical examination signs may overlap with ALD cirrhosis reflecting the presence of portal hypertension and its complications. Furthermore, the inflammation and steatosis of AH may promote de novo onset of portal hypertension in patients with minimal pre-existing liver disease and those with previously compensated cirrhosis. Signs of AWS may be present if cessation of drinking is recent (151). A careful search should be made for a source of potential infection or sepsis, including skin examination for signs of cellulitis and infection around venous lines. The systemic inflammatory response syndrome (SIRS 1”) (presence of 2 or more of temperature >38 or <36 degree Celsius, heart rate >90 bpm, respiratory rate >20 or PCO2 <32 mm Hg, and white cell count >12 × 109/L) may be present even in the absence of infection (152) and is associated with a nearly 3-fold risk of mortality (153). In addition, the presence of SIRS predicted the development of renal failure and 90-day mortality in 2 cohort studies (152,154).
Once a diagnosis of AH is made, disease severity is stratified. Although several scoring systems are available (155), the model for end stage disease (MELD) score is most frequently used to estimate disease severity and determine eligibility for corticosteroid treatment, with scores >20 indicating severe AH and ≤20 indicating moderate AH (156). These studies and recommendations are based on the original MELD and not MELD-sodium (MELD-Na) calculation (157). In one study, the MELD-Na score is as accurate in the assessment of disease severity and identifying patients eligible for corticosteroid treatment (158). It will be interesting to examine performance of MELD 3.0 in the assessment of patients with AH. Although the 90-day survival of patients presenting with severe AH has improved over time, current cohorts report a survival ranging from 35% (159) to 70% (160), with variability related to severity of AH and response to corticosteroids. The natural history beyond 90 days was highlighted in a single-center US study of 95 patients with severe AH with a median follow-up period of 795 days who were evaluated for, but ultimately did not undergo, LT. Spontaneous recovery (defined as having a MELD score of <21 at 90 days after the index hospitalization) occurred in 35% of individuals, but about half continued to have ascites and hepatic encephalopathy at the last follow-up. Only 7% of the cohort recovered to a compensated state (MELD <15 without ascites or hepatic encephalopathy) by the end of follow-up (161). For patients presenting with severe AH, hospitalization to determine clinical trajectory is preferable.
For patients with moderate AH, less is known about the natural history; however, the 1-year mortality ranges from 10% to 20% (162–164). In a study of all patients with AH, survival at 12 months among patients with moderate AH was 3-fold higher compared with those with severe AH (163). In another study of 142 patients with biopsy-proven AH followed for 55 months, lack of relapse to alcohol was associated with improved long-term survival (HR 0.53; P = 0.03) independent of MELD score (P < 0.05). Individuals who relapsed were of younger age (<48 years) and/or had a history of prior alcohol rehabilitation attempt (165).
Key concepts/statements
The Maddrey discriminant function index (mDF) is the historical index used to assess disease severity, corticosteroid eligibility, and short-term mortality risk in AH (166). Retrospective and prospective analysis of this score indicates that mDF ≥ 32 predicts a mortality rate of approximately 20%–50% over 30 days (167). Advantages of using the MELD score in the assessment of AH severity are its better accuracy, worldwide use in organ allocation, use of International Normalized Ratio over prothrombin time, and incorporation of serum creatinine, a major determinant of outcomes in patients with AH (156,168). A MELD score >20 has been proposed as defining severe AH with an approximately 20% 90-day mortality (156). Beyond MELD, other scoring systems that have been assessed for AH include Child-Turcott-Pugh, Glasgow Alcoholic Hepatitis Score (GAHS), and Age Bilirubin International Normalized Ratio and Creatinine (ABIC). In a post hoc analysis of 1,068 patients with AH in the steroids or pentoxifylline (PTX) for alcoholic hepatitis (STOPAH) study, mDF was inferior (receiver operating characteristic [ROC] 0.67) to MELD, GAHS, and ABIC scores (ROC 0.704–0.726) in determining short-term mortality at 28 and 90 days (169). In a prospective study on 71 biopsy-proven cases of AH, available scores (including MELD, GAHD, ABIC, mDF, and MELD-Na) were similar in accuracy, with 86%–100% ability to rule out severe disease, but had low positive predictive values ranging from 17% to 50% (158). Additional smaller studies have suggested that the performance of many scoring systems is similar in predicting 30-day mortality (170,171). Further analysis comparing several scores showed the MELD score to be the best score in assessing short-term mortality risk with ROC > 0.77 (157). Although MELD-Na and MELD are similar in predicting short-term mortality in AH (172), MELD 3.0 has been recently shown to have equivalent performance to MELD and may have utility to predict need for renal replacement therapy though further validation is needed (173).
There is a minimal role for liver biopsy for prognostication of AH. Although the Alcoholic Hepatitis Histologic Score, determined by presence and degree of bilirubinostasis, absence of megamitochondria, and degree of polymorphonuclear infiltration on biopsy (Figure 4), did reveal higher scores associated with higher 90-day mortality (174), the Alcoholic Hepatitis Histologic Score performed no better than GAHS and MELD scores in predicting 28-day mortality in the STOPAH cohort (175). Previous studies showed that the combination use of MELD at baseline and the Lille score at day 7 have best discrimination and calibration for 2-month and 6-month mortality (176).

Histologic features of alcoholic hepatitis: (a) circle represents lobular inflammation and arrow represents steatosis, (b) hepatocyte ballooning, (c) cholestasis with bile canalicular and hepatocyte plugging, (d) steatosis and fibrosis, (e) chicken wire and pericellular fibrosis, and (f) cirrhosis.
Patients with AH may present with ACLF as defined by various diagnostic criteria for ACLF, however, given the multitude of proposed scoring systems (177–180), lack of uniform definition across continents, and few studies limited to patients with AH, further work is needed to determine the optimal score for predicting mortality in AH patients with ACLF.
Recommendation
Infections are a common occurrence at presentation and during hospitalization in patients with AH. For example, in a prospective study of 1,092 patients with AH, 135 (12.4%) had an infection at baseline; of the remaining 957 patients, 251 (26.2%) developed infections during corticosteroid or pentoxifylline (PTX) treatment and 89 (9.3%) developed an infection after the treatment (181). In this study, prednisolone was associated with higher likelihood of infections after treatment but not during treatment and development of infection in those on steroids was associated with 2.46-fold higher 90-day mortality (181). However, in a meta-analysis of 12 other studies of 1,068 individuals with AH, the overall infection rate was 20% with no differences seen in those who received corticosteroids or not, although a higher risk specifically for fungal infections was found in steroid-treated patients (182). Another multicenter retrospective cohort study of patients with AH found that 49% had evidence of infection and the diagnosis of infection was an independent risk factor for 90-day mortality (HR 2.33, 95% CI 1.63–3.35, P < 0.001). In this study, however, initiation of empiric antibiotics on admission in the absence of infection did not reduce mortality or alter the incidence of subsequent infections. Corticosteroid use increased the incidence of infection, but this did not affect survival (183).
Studies on the use of prophylactic antibiotics in patients with AH have not shown promise for mortality benefit. In a placebo-controlled trial, rifaximin use for 90 days in patients with AH safely reduced infections (0.29 vs 0.62 infections/patient) and liver-related complications (0.43 vs 1.26 complications/patient) and showed a trend for lower 90-day mortality compared with the control arm (184,185). However, a 7-day course of oral vancomycin, gentamycin, and meropenem in 14 patients with AH showed no 90-day survival benefit compared with a reference group of patients with AH receiving standard of care (186). In the Antibiocor trial, 284 individuals with biopsy-proven AH were randomly assigned to receive prednisolone plus amoxicillin/clavulanate or prednisolone plus placebo for 30 days. Those in the antibiotic group had a lower cumulative incidence of infection (42 vs 59 events; HR 0.616, P = 0.015), but there was no difference in 60-day mortality (24 vs 31 in deaths; HR 0.769; 95% CI 0.451–1.31).
Recommendation
Key concepts/statements
Severe malnutrition is common in individuals with severe AH and portends a worse short-term survival (187–191). Although low caloric intake (<21.5 kcal/kg/d) is associated with increased risk of 28-day mortality (192), the caloric intake goal of 35 kcal/kg/d with 1.2–1.5 g/kg of protein for people with AH is based on work in populations with critical illness and not necessarily AH (148). The most beneficial route of feeding remains unclear and is generally tailored to a patient’s ability to safety eat by mouth. A randomized study of enteral feeding compared with oral feeding in 136 biopsy-proven patients with severe AH showed no difference in survival; however, a caloric intake of <21.5 kcal/kg/d irrespective of the trial arm was associated with higher mortality at 6 months (62.9 vs 34.2%, P < 0.001) (192). Similarly, the efficacy of enteral feeding as an intervention compared with steroids in 71 patients showed noninferiority for short-term (28-day) survival, but deaths occurred earlier in the enteral feeding arm (193). In a small trial comparing nasogastric with nasojejunal tube feeding, there was no difference in the amount of successfully delivered daily calories (194). It should be noted that feeding tubes can be safely placed in patients with esophageal varices without active bleeding or who have not undergone recent endoscopic variceal banding (195). In those who cannot eat by mouth or have a contraindication to enteral feeding, total parenteral nutrition may be used. Total parenteral nutrition has no short-term survival advantage when compared with oral and enteral feeding in moderate or severe AH (196).
Amino acid supplementation has been studied in patients with AH with mixed results. In a small, 28-day study of patients with AH provided a 3,000 kcal diet with 100 g protein, those who received 70–85 g of IV amino acids daily had a 100% 28-day survival, whereas those who did not had a survival rate of 78% (197). Several subsequent studies of daily amino acid supplements (mixed and branch chain) found no survival benefit in AH (198–200). Vitamin and mineral deficiencies are also common in patients with AH. As patients with AH have recent harmful alcohol use, supplementing with thiamine may help prevent Wernicke encephalopathy (148). However, a meta-analysis of various mixed nutritional supplements (amino acids, vitamins, minerals, and lipid) found no mortality benefit in AH (201). Supplementing select trace elements may be considered. A recent study found that 85% of patients with AH are zinc deficient, and zinc deficiency was an independent predictor of 28-day mortality with an odds ratio of 10.6 per 1 μmol/L decrease in serum zinc level (202). Although zinc supplementation has been included as an intervention for AH in clinical trials (203), studies of the therapeutic effect of zinc alone are limited.
Recommendation
Key concept/statement
Corticosteroids
The first randomized controlled study to assess efficacy of corticosteroids in the treatment of AH was published in 1971 (204). A Cochrane review of 16 randomized controlled studies showed no difference between corticosteroids and placebo (or no intervention) on all-cause mortality, health-related quality of life, and serious adverse events, although the quality of evidence was classified as very low or low (205). In a pooled analysis, using individual level data from the 5 largest randomized controlled studies (193,206–209), corticosteroids provided a survival benefit at 28 days (80% vs 66%, P < 0.0001) (210). The largest single randomized, placebo-controlled multicenter study from the United Kingdom (the STOPAH study) of 1,103 patients with severe AH randomized to 28 days of prednisolone or placebo showed only a trend for mortality benefit (13.8% vs 18%, P = 0.056) and an overall lower frequency of mortality in this cohort than previous studies (160), likely reflecting improved management of advanced liver disease. Finally, an updated meta-analysis of more contemporary randomized studies (including the STOPAH study) showed that corticosteroids were effective in reducing short-term mortality by 36% (211).
Given the variable severity of individuals presenting with AH, corticosteroids may be more effectively used if targeted to those most likely to respond, with early cessation of steroid therapy in those unlikely to response. A recent worldwide retrospective multicenter cohort of individuals with severe AH demonstrated that the 28-day corticosteroid survival benefit is seen in those with MELD scores ranging from 21 to 39, with limited benefit in the 40–50 range and no benefit with MELD scores above 50 (74). The Lille score at day 4 of corticosteroid therapy has been shown to be as accurate as day 7 Lille score in predicting the outcome and response to treatment (212) and has since been validated (213). Predicting which individuals will have a spontaneous recovery without steroid use is of great interest given the side effect profile. In a recent study of 426 patients with AH, the trajectory of serum bilirubin over the course of admission was categorized into “fast fallers,” “static,” and “rapid risers.” Fast fallers (those with a bilirubin <0.8 × admission value at day 7) had superior 90-day survival. In these individuals, use of corticosteroids showed no benefit (214).
Prednisolone has been more extensively studied and is generally used over prednisone. Prednisolone and prednisone are dosed 40 mg per day for a total duration of 4 weeks (Figure 3). IV methylprednisolone (32 mg per day) is an alternative for those unable to take medications orally. There is no evidence supporting the benefits of rapid vs slow tapering after the 4-week therapy.
Active infection including untreated HBV infection, uncontrolled diabetes mellitus, gastrointestinal bleeding, and severe renal failure is considered contraindications to the use of corticosteroids (215). However, corticosteroids can be started after adequate control or reversal of infection, renal failure, and gastrointestinal bleeding. For example, use of corticosteroids after adequate control of infection has been reported to provide benefit (216). Development of infections remains a concern among those treated with corticosteroids (217), particularly the risk of fungal infections (182). In the STOPAH study, use of prophylactic antibiotics as an adjunct to corticosteroids improved patient survival in those with adequate treatment of baseline infection and in those with a baseline bacterial DNA level of >18.5 pg/mL (181). Prophylactic amoxicillin/clavulanate in a recently concluded randomized clinical trial as an adjuvant to prednisolone-reduced infection however did not improve patient survival (218).
Recommendations
Pentoxifylline
PTX is a phosphodiesterase inhibitor and inhibitor of tumor necrosis factor-α (TNF-α), one of the major cytokines speculated in the pathogenesis of AH (219,220). Despite the first seminal study showing benefit of PTX 400 mg 3 times a day for 28 days (221), there was no survival benefit in the STOPAH study (160). The most promising data for PTX were not effective in reducing the short-term mortality at 28 days (222). In addition, PTX was not effective as a salvage option for steroid nonresponders (223). In a meta-analysis of 10 randomized studies, PTX failed to show survival benefit at 1 month but was effective in reducing the occurrence of hepatorenal syndrome by 53% (224). In a network meta-analysis of 22 studies including the STOPAH study, there was low-quality evidence for benefit of PTX in reducing the short-term mortality at 28 days by 30% (222). In addition, PTX was not effective as an adjuvant therapy to corticosteroids (225,226). The exact mechanism of renal protection with PTX remains unclear.
G-CSF
G-CSF is proposed to have regenerative liver effects and has been studied in patients with severe AH deemed steroid ineligible or nonresponsive. Subsequently, meta-analyses have examined the efficacy of G-CSF in AH with 5 studies in Asia showing a 90-day survival benefit and 2 studies in Europe showing no survival benefit but rather a trend to increased mortality. It has been proposed that study design variability accounted for mixed results (227,228). The combination of G-CSF and prednisolone has also yielded mixed results with a recent US trial showing equivalent 90-day survival to prednisolone (0.73 [95% CI 0.44–0.89] vs 0.83 [95% CI 0.57–0.94]; P > 0.05) (229), while a study from Asia (NCT04066179) comparing G-CSF alone (N = 42), prednisolone alone (N = 42), and the combination of G-CSF + prednisolone (N = 42) showed 64.3%, 78.6%, and 88.1% 90-day survival, respectively (P = 0.03) (230). Further studies are needed to determine whether G-CSF, alone or in combination with corticosteroids, has efficacy in decreasing mortality in AH.
N-acetyl cysteine
N-acetyl cysteine (NAC) has proven benefit in acetaminophen toxicity and was initially studied in AH in combination with other antioxidants without observed benefit (231). Furthermore, monotherapy NAC infusion (vs placebo) over 14 days did not show any survival benefit at 1 and 6 months (232). Two studies evaluating NAC as an adjuvant to prednisolone showed divergent results, with one showing improved survival at 1 month (but not at 3 and 6 months) (233) and another without 30-day survival benefit (234). Both studies were of modest sample size and had differences in MELD scores between treatment groups (29.2 ± 6.3 vs 25.5 ± 6.4, P = 0.03) (234) limiting interpretation. A network meta-analysis comparing various pharmacological agents showed moderate quality evidence that a combination of prednisolone and 5 days of NAC infusion provides the best survival benefit at 28 days with 85% risk reduction of death from AH (222). Based on this evidence and considering its excellent safety profile, ACG has recommended that IV NAC may be used as an adjuvant to steroids; however, other society guidelines have not included such a recommendation. Additional clinical trials are ongoing.
Anti-inflammatory drugs
Based on preclinical efficacy and beneficial effects in open label trials, TNF inhibitors were initially promising; however, randomized trials in severe AH were terminated early because of a higher number of deaths in treatment arms, with most deaths due to infections (235,236). The mechanisms of these findings are believed to be due to blockade of the beneficial effects of TNF on hepatic regeneration (237). Results of a trial comparing methylprednisolone (28 days) with a combination of the IL-1 receptor antagonist anakinra (14 days) plus PTX (28 days) plus zinc (180 days) for the treatment of severe AH showed no survival difference at 28, 90, or 180 days (203).
Microbiome modulation
Despite enthusiasm for probiotic use, data are lacking regarding benefits in AH, with studies limited by small sample size and lack of inclusion of patients with severe AH (238–240). The first fecal microbiota transplantation (FMT) trial in 8 subjects with AH having contraindications to steroid therapy showed encouraging results (241) and has since been followed by a randomized controlled trial comparing FMT (N = 55) with prednisolone (N = 57) with improved 90-day survival in the FMT arm compared with the prednisolone arm (75% vs 57% P = 0.044) (242). Although fewer infections were seen in the FMT arm of the aforementioned study, given the relative immunocompromised status of patients with severe AH, the risks and benefits of FMT must be considered because infections from donor stool have been reported (243) leading to several US FDA alerts in the past few years. Clinical trials of FMT for the treatment of AH are ongoing.
Miscellaneous therapies
Antioxidant cocktails and vitamin E have not shown benefit in severe AH (209,231,244). The antioxidant S-adenosylmethionine, when added to prednisolone, showed no 28-day survival benefit over prednisolone alone; however, there were fewer cases of hepatorenal syndrome observed with the antioxidant arm (245). Hepatic regenerative capacity supported by bone marrow-derived stem cells and hepatic progenitor cells seems clinically important (246,247). However, drugs targeting this capacity including insulin and glucagon (248,249), the anabolic steroid oxandrolone (250), and propylthiouracil (251) have not demonstrated mortality benefit. The molecular adsorbent recycling system safely improves cholestatic pruritus and renal function without any significant improvement in survival (252). Furthermore, a preliminary report of plasma exchange in a randomized trial of 50 patients with ACLF showed improved 1-year survival; however, it was unclear how many of these patients had AH (253).
Clinical trials
Active studies for AH including therapeutics targeting hyaluronic acid (NCT0501848) and epigenetic pathways using an endogenous sulfated oxysterol, larsucosterol (NCT04563026), and IL-1 inhibition (NCT03775109) are in progress.
LT
Recommendation
Key concept/statement
Retrospective and prospective studies have established a survival benefit in offering LT to appropriately selected patients with severe AH unresponsive to or with contraindications to corticosteroids. The initial landmark study on 26 patients with severe AH unresponsive to corticosteroids who were selected to receive LT without a mandated period of sobriety had a 2-year survival of 72% compared with 24% survival in patients with severe AH not eligible for LT (254). A larger prospective multicenter Franco-Belgium study (QUICK-TRANS) evaluated survival and alcohol relapse among those with severe AH who did not respond to medical management and who were evaluated for LT using an objective score based on standardized selection criteria (159). Patients with a score of >220 of a maximum score of 250 selected for LT (early LT group, N = 102) were compared with patients not eligible for LT (non-LT group, N = 47) and with patients with ALD cirrhosis listed for LT after at least 6 months of abstinence (standard LT group, N = 127) (159). After 2 years of follow-up, posttransplant survival was similar between the early LT group and the standard LT group (HR 0.87, 95% CI 0.33–2.26) but was significantly higher compared with the non-LT group (HR 0.27, 95% CI 0.16–0.47). In a large multicenter retrospective US study (American Consortium for Early Liver Transplantation [ACCELERATE]-AH) of 147 patients with severe AH unresponsive to medical management, 3-year patient survival was 84%, similar to historical controls with ALD cirrhosis with mandated sobriety periods (83%) (11,255). Several subsequent retrospective and small prospective studies have confirmed that outcomes of early LT in patients with severe AH are similar to LT for ALD cirrhosis with mandated periods of abstinence (256,257). In a meta-analysis of 11 studies on LT for ALD, the pooled patient survival rate at 6 months was 0.85 (95% CI 0.77–0.91) and 0.80 (95% CI 0.69–0.88) among patients receiving early LT for severe AH (257).
Key concepts/statements
In a meta-analysis of 11 studies on LT for ALD, including those with AH, the pooled alcohol use recurrence rate was 0.22 (95% CI 0.12–0.36) and 0.20 (95% CI 0.07–0.43) in a subgroup of patients with severe AH receiving early LT, OR = 1.68 (95% CI 0.79–3.58, P = 0.2) (257). The rates of alcohol relapse among recipients of LT for AH were evaluated prospectively in the QUICK-Trans study using the timeline follow-back survey (159). The rate of relapse was not significantly different between the early vs standard LT (≥6 months sobriety) groups (34% vs 25%; P = 0.45) at 2-year follow-up, although the rates of high alcohol intake were greater in the early LT group (absolute difference 16.7%, 95% CI 5.8–27.6). In the ACCELERATE-AH cohort, where biomarker testing was used to supplement assessment of alcohol relapse, the cumulative incidence of any relapse was 25% (95% CI 18%–34%) at 1-year and 34% (95% CI 25%–44%) at 3-year post-LT, with the cumulative incidence of sustained alcohol use being 10% at 1-year (95% CI 6%–18%) and 17% at 3-year (95% CI 10%–27%) post-LT (258). Early onset (<1-year post-LT) and heavy patterns of alcohol use are associated with reduced post-LT survival (258–260) among patients transplanted for AH.
Although length of abstinence predicts alcohol use after LT, other factors such as untreated psychiatric disease, history of polysubstance abuse, history of legal consequences related to alcohol use, lack of insight, lack of willingness to engage in AUD treatment, multiple prior failed rehabilitation attempts, and lack of social support are stronger variables associated with recurrent alcohol use after LT (261). Furthermore, a recent study showed 3-year patient survival rates after LT to be lower in those with a history of decompensation vs first episode (72% vs 83%, P = 0.01) (262).
Selection of patients with severe AH for LT requires a rigorous psychosocial evaluation by a multidisciplinary team including social workers and addiction counselors and psychiatrists. Tools such as Stanford Integrated Psychosocial Assessment Tool (261,263), High Risk for Alcohol Relapse Score, Michigan Alcoholism Prognostics Score, Hopkins Psychosocial Score, and SALT score may be used to determine risk of recurrent alcohol use after LT (100,264,265). However, most of these scores are not accurate in identifying patients who are at high risk for recurrent alcohol use but rather are accurate in predicting a low likelihood of relapse. For example, the SALT score has a negative predictive value of 90%–95% (not likely to have recurrent alcohol use after LT) but a positive predictive value of only 25%–50% (likely to have recurrent drinking) (266). This was also exemplified in the recently reported data from the QUICK-TRANS study, with harmful alcohol use at 2-year follow-up of 22% in the early LT group compared with 5.4% in the standard LT group, despite an objective score used for listing with 200 of 250 points in the score ascribed to detailed psychosocial evaluation (159). Alcohol biomarkers can be used to supplement self-reported information for accurate detection of alcohol use among patients waitlisted for better selection of those who ultimately end up receiving LT. Biomarker use should be ethical and transparent because positive biomarkers may have a long-lasting stigmatizing effect on patients with ALD and may also lead to decreased access to LT (267,268). Clearly, there remains an unmet need in the field for accurate, objective tools for patient selection for early LT in patients with ALD.
Key concepts/statements
Patients waiting on the transplant list should be monitored for alcohol consumption because approximately 17%–30% of these patients may relapse to alcohol use (269,270). When integrated into transplant center protocols, biomarkers can detect harmful drinking where relapse to alcohol can significantly harm the allograft and lead to decreased posttransplant survival (258,259). Postliver transplant, approximately 30%, will experience a slip or sustained alcohol use within a follow-up period of 2 years (159,258,259). As AUD is a chronic disorder, strategies to reduce risk of relapse are highly recommended. An integrated multidisciplinary care model for LT candidates and recipients should be the goal, with hepatologists providing liver-focused care and addiction specialists providing AUD-focused care, longitudinally. In a prospective, noncontrolled pilot program assessing a multidisciplinary care model for AUD in the pretransplant and posttransplant care of patients with <6 months of sobriety before LT, only 3 of 44 patients relapsed to alcohol use (mean follow-up period = 339 days) (271). In a meta-analysis of 6 studies on 649 patients transplanted for ALD, a multidisciplinary integrated care model compared with follow-up by hepatology alone in a transplant clinic was associated with lower rates of relapse to alcohol use and long-term patient mortality, with the respective odds ratio of 0.56 (95% CI 0.36–0.87) and 0.29 (95% CI 0.08–0.99) (137). Use of medications to reduce cravings may be considered, although there are no studies of the efficacy of medication-associated therapy in liver transplant recipients.
Key concept/statement
Alcohol use affects long-term survival of LT patients because those with early, sustained nonheavy use and early, heavy use (binge drinking or frequent drinking defined as drinking 4 or more days in the week) have a significantly lower 3-year survival compared with those who remained abstinent or have late, nonheavy use: 81% vs 53% vs 99%–100% (P < 0.001) (258). In a meta-analysis of 7 studies for alcohol-associated cirrhosis, the pooled annual alcohol recurrence rates were 4.7% (3.0%–6.4%) for any alcohol use and 2.9% (0.5%–5.3%) for harmful alcohol use. Among recipients needing a liver biopsy for their clinical care, those with recurrence of alcohol use compared with abstainers had increased odds for steatohepatitis (OR 4.5, 95% CI 1.4–14.2), AH (OR 9.3, 95% CI 1.01–85), and advanced fibrosis or cirrhosis (OR 8.4, 95% CI 3.5–20). Furthermore, mortality at 10 years after LT was over 3-fold higher among recipients with recurrent alcohol use compared with abstainers (OR 3.67, 95% CI 1.42–9.50) (259). Recurrent alcohol-associated cirrhosis occurring in 9% of biopsied patients and 2% of all transplants was responsible for approximately 20% of posttransplant deaths. Early onset (<1-year post-LT) and heavy patterns of alcohol use are associated with reduced post-LT survival (258–260) among patients transplanted for AH.
PUBLIC POLICY AND PREVENTION
Key concept/statement
Policy measures aimed at reducing alcohol use include taxation, reduced availability, and restricted promotion of alcohol-containing beverages. Effective alcohol policy measures have been shown to reduce alcohol-related mortality, including ALD-related mortality (272,273). Cost-effective measures include increase in taxes on sales of alcohol, alcohol marketing restrictions including ban on advertising alcohol on public platforms, raising the legal age for alcohol purchases, psychosocial interventions from clinicians, limitations on public drinking, and stricter legal consequences for driving while intoxicated (274). In the United States (275) and Latin America (276), strict alcohol policy environments, especially alcohol taxes, were associated with lower ALD cirrhosis mortality rates. Benefits to society, however, can take years to realize after policy change. A recent US study revealed that states enacting stricter alcohol policies experienced declines in ALD mortality, with the mortality effect lagging 5 years after policy change (277). Associations between tariffs on alcohol and rates of hospitalizations for AH and LT for ALD suggest that public health benefits can be achieved by excise taxing of alcohol (278). The effect of cold climate and limited daylight hours on escalated alcohol drinking have been reported (279) and may help to inform geotemporal alcohol policy efforts. Education is an important supplement to public policies noted above but may be less effective in the absence of policy interventions. Examples of education include youth-focused education in school, after-school programs, and parental education. Population-based screening tools and algorithms may also be effective to identify AUD and diagnose ALD at a population level.
CONCLUSIONS AND PROSPECTS
Healthcare burdens from AUD and ALD are significant in the United States and worldwide and are increasing in recent years. Providers in all clinical areas must be prepared to care for this growing population of patients. Patients with ALD often present at an advanced stage are rarely offered AUD treatment and have few effective therapies aimed at their liver disease. With continued and increasing interest of researchers and funding organizations especially the NIAAA, there seems light at the end of the tunnel with a promising future to fill the knowledge gap in several unmet clinical needs in the field of ALD (Table 6). Policy aimed at alcohol use reduction, multidisciplinary care of the dual diagnoses of AUD and ALD, and refinement of LT algorithms for patients with severe AH are areas where research should be focused.

Prospective areas of clinical-translational research
CONFLICTS OF INTEREST
Guarantor of the article: Vijay H. Shah, MD.
Specific author contributions: All the authors wrote different key portions of these guidelines, were involved in regular teleconferences with the guideline committee members for making appropriate revisions, and all approved the final document.
Financial Support: NIH U01 AA021788 (V.H.S.), NIH K08DK123381 (L.L.J.). American College of Gastroenterology Faculty Development grant, NIH R21 AA023273 (A.S.) and NIAAA 1U01AA021908-01 (R.B.).
Potential competing interests: Echosens (R.B.); Novartis, Merck, Durect (V.H.S., N.A.T.); Abbvie, Galectin, Bausch/Salix, Aldeyra (L.L.J.); Pleiogenix Pharmaceuticals and Durect Pharmaceuticals (A.S.).
ACKNOWLEDGMENTS
This guideline document was developed in collaboration with the practice guideline committee of the American College of Gastroenterology. We acknowledge and thank the services of Leslie Hassett, MLS, for the systematic literature search and Theresa Johnson (both of Mayo Clinic) for administrative assistant support.
REFERENCES