Cost of Care for Patients With Cirrhosis : Official journal of the American College of Gastroenterology
INTRODUCTION
Cirrhosis of the liver is a common condition with documented gaps in health care delivery (1,2). Substantial efforts are underway to improve the quality of health care for patients with cirrhosis (3,4). To guide value-based care efforts, health care leaders also need estimates of cirrhosis costs (5). To be most useful, cost estimates should encompass the whole course of care from diagnosis to ongoing management. While many studies have examined other outcomes of patients with cirrhosis, few have quantified the costs required to deliver those outcomes, and even fewer in a longitudinal cohort that allows comparison with national averages (6–8). Most previous studies of cirrhosis cost focused on end-of-life or inpatient cohorts, limiting their utility in focusing value-based improvement initiatives.
As an end-stage organ disease, cirrhosis has many causes, and different underlying etiologies may have different costs over the course of care. However, few studies have examined the costs of managing patients with different cirrhosis etiologies. Cirrhosis also causes a range of complications, including ascites, hepatic encephalopathy, variceal bleeding, hepatocellular cancer (HCC), and acute kidney injury (AKI). Each of these complications may affect health care utilization and costs differently. Information about cost of patients with compensated and decompensated cirrhosis can help target value improvement efforts. Similarly, patients with cirrhosis often have significant mental health and other comorbidities. Understanding the relationship of those comorbidities to costs can inform decisions about resource allocations and case-mix adjustment algorithms (9–12). We conducted a retrospective longitudinal cohort study of patients with cirrhosis. We compared their long-term costs and resource use with matched controls over the course of care.
METHODS
Data source
We used data from national Veterans Administration (VA) Corporate Data Warehouse, which includes laboratory test results, pharmacy, and inpatient and outpatient procedure (Current Procedural Terminology codes) and diagnosis codes (International Classification of Diseases, Ninth/Tenth Revision [ICD-9/ICD-10]). Corporate Data Warehouse also hosts Vital Status and VA Purchased Care; the latter includes services rendered outside the VA but paid by the VA. We extracted cost data from the VA Managerial Cost Accounting system, an activity-based accounting system within the VA, and the Purchased Care data.
Cirrhosis cohort
We included patients with new diagnosis of cirrhosis who were seen at 130 VA hospitals from January 10, 2011, to September 30, 2015. We included patients if they had at least 2 instances of cirrhosis or cirrhosis complications codes in the inpatient or outpatient settings or at least 1 code for cirrhosis or complications with at least 1 filled prescription of spironolactone (100 mg for ascites), rifaximin, or lactulose (for encephalopathy) after a cirrhosis diagnosis (eTable 1, Supplementary Digital Content 1, https://links.lww.com/AJG/D24). These algorithms had high positive predictive value (86%–93%) for the presence of cirrhosis in patients’ medical records (1,8). We selected the first cirrhosis diagnosis date as the index (entry) date for follow-up.
Control cohort
We selected controls from individuals who did not meet cirrhosis criteria but had a visit to the VA between January 10, 2011, and September 30, 2015. We used random sampling without replacement to select controls matched for gender, hospital, year of index visit (using 2-year intervals), and age at index (using 5-year age groups). We also matched patients on duration from their first VA visit to the index visit to ensure equal ascertainment of clinical and health care utilization covariates. We selected up to 4 controls for each patient with cirrhosis. For our cohorts, we acquired data through September 30, 2019, to ascertain cost and utilization.
Variable selection
Dependent variable.
Our primary outcome was total cost for each of the first 4 years after cirrhosis diagnosis (eTable 2, Supplementary Digital Content 1, https://links.lww.com/AJG/D24). To do so, we grouped costs over time into 1-year intervals from study entry. We examined the marginal effect of cirrhosis diagnosis on the subtypes of cost (outpatient, inpatient, pharmacy, and purchased care) separately and then summed the results to obtain an overall estimate. Confidence intervals (CI) were constructed by calculating a pooled variance across the different components. We converted costs to 2019 US dollars using the Personal Consumption Expenditures price index constructed by the US Bureau of Economic Analysis (13).
In addition, we examined number of inpatient, emergency department, and outpatient encounters overall and by specialty (primary care, gastroenterology, other specialties), number of tests, procedures, and prescriptions. We defined outpatient encounters as the number of unique calendar days on which an outpatient visit occurred. We obtained all-cause mortality data from VA Vital Status file (14).
Predictor variables.
For both cases with cirrhosis and matched controls, sociodemographic variables included age, sex, race, medical insurance status, and enrollment priority level. We classified insurance as VA-private, VA-public (Medicare or Medicaid), and only VA insurance. Priority level is a VA-specific variable based on military service history, income, service-connected disability, and eligibility for government aid (15,16).
At least 40% of patients with cirrhosis have comorbidities that increase health care costs. We used ICD-9/10 codes to derive the Deyo comorbidity index (17). Other health conditions included depression and anxiety. Last, we included history of prior hospitalization, number of outpatient visits (count), and duration of time in VA care before the index visit for both cases and controls.
We defined hepatitis C virus (HCV) based on any evidence of positive HCV ribonucleic acid test, HBV based on any positive hepatitis B surface antigen (18), and alcohol-related liver disease based on ≥1 instance of an ICD-9/10 code for alcohol use disorders any time before index visit. We identified nonalcoholic steatohepatitis (NASH) as the possible etiology of cirrhosis for patients without any other cause who had type 2 diabetes or body mass index of greater than 30 kg/m2 before diagnosis of cirrhosis (19).
We extracted automated data from serum bilirubin, international normalized ratio, and sodium and creatinine tests performed within 1 year before and closest to the start of the given year and combined them to derive laboratory Model for End-Stage Liver Disease-Sodium (MELD-Na) scores (1). We also defined type of cirrhosis complications (ascites, hepatic encephalopathy, variceal bleeding, or HCC) at baseline and during each year of follow-up based on ICD codes recorded within 6 months after start of each year. Among the subgroup of patients who were hospitalized during the first 6 months of each yearly interval, we defined AKI based on ICD-9 codes and/or if patients had either ≥0.3 mg/dL or 50% increase in serum creatinine, as previously described (20).
Statistical analyses
We grouped costs over time into 1-year intervals from the time of study entry. We included cases (and their corresponding controls) if they were alive at the beginning of that year for each yearly interval. Some patients could have died during the course of the year, often after incurring high costs in the last months of life. While our primary cost estimates reflect this experience, they might not accurately capture the costs of survivors. Hence, we also calculated conditional mean costs for patients who survived the full-year interval as part of a sensitivity analysis.
Because a substantial proportion of patients did not incur any outpatient (3.5% of cases and 20% of controls) or inpatient costs (67.3% of cases, 95.2% controls), we used 2-part regression to model cost outcomes: (i) probability of incurring any costs vs none and (ii) continuous cost (conditional on nonzero costs) (21,22). Part 1 of the 2-part model was performed using logistic regression while part 2 used a generalized linear model. We determined gamma was the most fitting distribution for the cost data using the modified Park test (23). The results are presented as marginal effects across the 2 models to make inferences across the entire cohort (21,24–26).
We also conducted several subgroup analyses to understand the main drivers of costs, including cirrhosis etiology (HCV, alcohol, HCV and alcohol, NASH, other etiologies), severity (MELD-Na categories), complications (compensated, decompensated cirrhosis and individual cirrhosis complications), and comorbidity (Deyo index, mental health comorbidity). Some patients with dual health insurance may seek care outside the VA, and this could influence the incremental cost estimates, especially if such use was more common among patients with cirrhosis (e.g., care at a non-VA liver transplant center). We stratified analyses by insurance status to determine whether our results were sensitive to care that could have been delivered outside the VA.
Last, as a secondary analysis, we compared the cost of caring for patients with cirrhosis with the cost of caring for patients with 2 other common chronic conditions, chronic obstructive pulmonary disease (COPD) and congestive heart failure (CHF). To do this, we identified patients with COPD or CHF from among our cohort of control patients using ICD codes. We maintained the case-control matching, where each cirrhosis control was compared with his/her matched COPD or CHF control, and used 2-part models (as described earlier) to estimate the marginal effects.
RESULTS
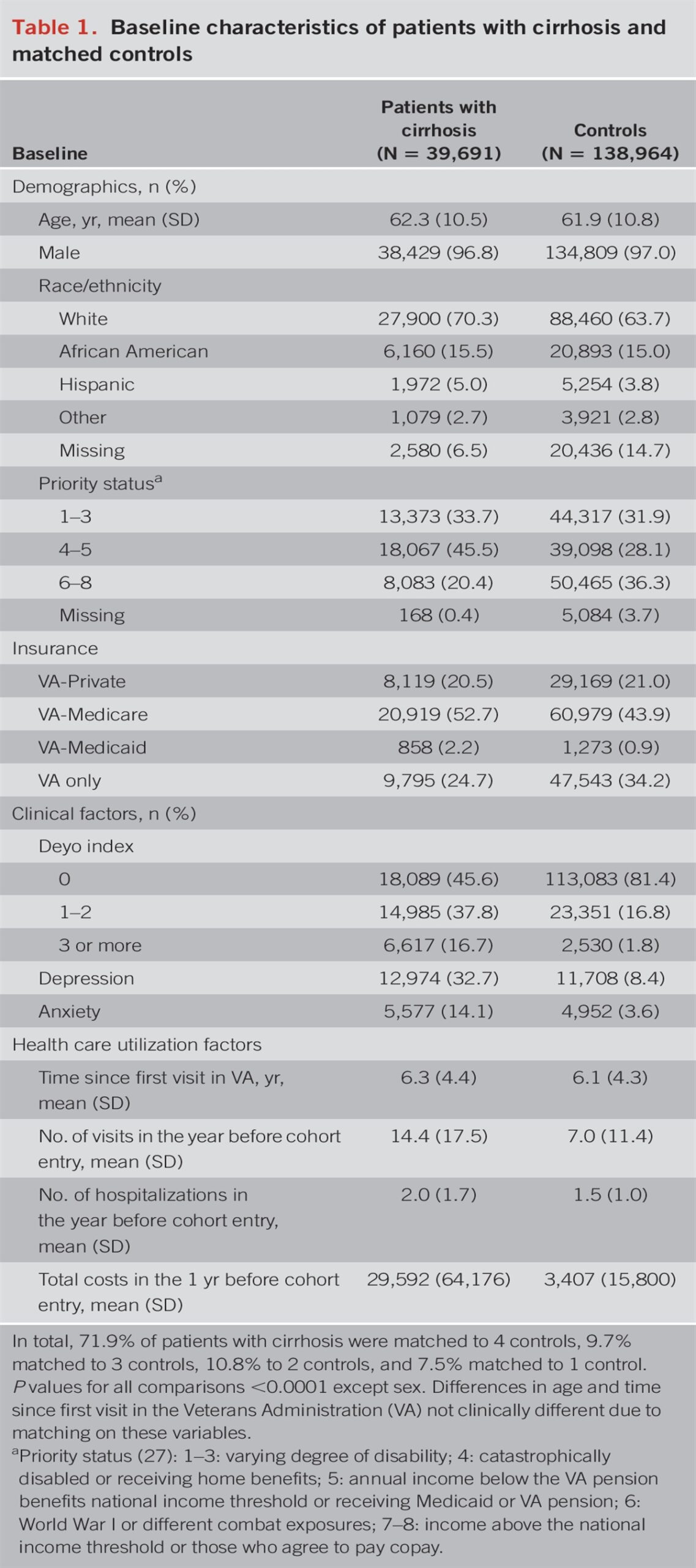
We identified 39,691 patients with cirrhosis and 138,964 matched controls (Table 1). The mean (SD) age of patients with cirrhosis was 62.3 (10.5) years, 96.3% were male, 70.3% were White, 15.5% were African American, and 5.0% were Hispanic.

Baseline characteristics of patients with cirrhosis and matched controls
Of the patients with cirrhosis, 20.5% had VA-private insurance, 52.7% had VA-Medicare, and 24.7% had VA as the only source of medical insurance. In total, 16.7% had significant multimorbidity (defined as Deyo index of 3 or more), 32.7% had depression, and 14.1% had anxiety. Most patients had either alcohol-related (32.7%) or HCV-related (HCV alone or in combination with alcohol, 30.2%) cirrhosis; 11.6% had NASH cirrhosis. Approximately 39.0% of year 1 cohort had cirrhosis complications (defined as either ascites, hepatic encephalopathy, or varices) and 18% had AKI (Table 2). Most of the patients had 1 complication, likely related to the fact that the cohort included newly diagnosed patients; 6% had more than 1 cirrhosis complication.

Liver disease–related characteristics of patients with cirrhosis at index diagnosis
Compared with matched controls, patients with cirrhosis were significantly more likely to be older, more likely to be of lower income status (priority status 4–5), had higher burden of comorbidity, and had greater health care utilization within 1 year before cohort entry (all P values <0.0001, Table 1).
The mean durations of follow-up for the cirrhosis and control cohorts were 3.7 (SD 2.5) and 5.6 (SD 1.7) years, respectively. In total, 24.9% of patients with cirrhosis died within the first year followed by an annual mortality rate of 8.1%–10.6% in the subsequent years, with cumulative all-cause mortality of 43.9% at 4 years. By contrast, cumulative all-cause mortality among controls was 2.7% at 1 year, 4.3% at 2 years, 5.6% at 3 years, 6.9% at 4 years.
Costs and resource use
The mean cumulative costs for patients with cirrhosis were significantly higher than the costs for matched controls at 1 year ($57,544 vs $9,603) (Table 3). The mean cost of care for patients with cirrhosis for the subsequent 3 years ranged from $32,930 to $36,374 per patient per year. After accounting for differences in age, gender, race/ethnicity, priority status, health insurance status, and baseline health care utilization, the incremental first year cost of caring for patients with cirrhosis was $45,839 (95% CI 4$2,862–$48,817). The incremental cost was lower after additional adjustment of comorbidity ($35,029, 95% CI $32,473–37,585) (Table 4). The full model is summarized in eTable 3 (Supplementary Digital Content 1, https://links.lww.com/AJG/D24). While the first year was the costliest, the difference in cost between patients with cirrhosis and controls was positive and significant for years 2–4 as well ($17,629–$14,216). The 4-year cumulative cost difference was $71,061 ($65,393–$76,730). In the sensitivity analysis conditional on survival, economic burden of cirrhosis remained appreciable, though total inpatient costs of managing patients with cirrhosis were lower in this sensitivity analysis compared with those in the primary analysis, demonstrating the high economic burden associated with the last weeks of life (eTable 4, Supplementary Digital Content 1, https://links.lww.com/AJG/D24). The incremental cost of cirrhosis was similar and remained high across the subgroups defined based on health insurance status (VA only insurance, VA-Medicare, and VA-Private insurance, eTable 5, Supplementary Digital Content 1, https://links.lww.com/AJG/D24).

Health care utilization among patients with cirrhosis and matched controls

Incremental cost of cirrhosis overall and by type of health care expenditure: results from multivariable models
The elevated total costs were mostly due to higher inpatient costs (Table 4), which were driven both by a greater number of hospitalizations and longer average length of hospital stay for patients with cirrhosis (Table 3). Patients with cirrhosis also had significantly more emergency department visits, primary care encounters, gastrointestinal encounters, and outpatient visits relative to control patients (P < 0.0001). In addition, procedure use was higher in patients with cirrhosis, with significantly more imaging tests and endoscopy procedures, as was the number of days in the intensive care unit compared with that in controls.
Development of decompensated cirrhosis resulted in a sharp increase in medical costs (incremental cost of $50,362) in the first year, but this cost stabilized by the second year (Figure 1). Cost of managing patients with hepatic encephalopathy (year 1 cost, $50,080, 95% CI $41,436–$58,724) was similar to that of managing patients with ascites (year 1 cost, $50,364, 95% CI $41,748–$58,980), both higher than the cost of managing patients with varices (year 1 cost, $20,488, 95% CI $13,762–$27,215). In years 2–4, the incremental costs of caring for patients with HCC (years 2–4 incremental cost, $86,741) exceeded those of managing other complications (years 2–4 incremental costs for patients with ascites and encephalopathy were $49,223 and $49,529, respectively). The incremental cost was the highest for caring for patients with AKI (year 1 cost, $64,413, 95% CI 55,929–$72,896). Patients with cirrhosis with significant multimorbidity (defined as Deyo index of 3) were the costliest with year 1 incremental cost of $66,653 (95% CI $56,539–76,768). For the 32% of patients with cirrhosis and depression, the incremental cost was $44,778 compared with $34,061 for patients without depression. The incremental cost was similar among patients with cirrhosis from different etiological risk factors (Figure 1).

Incremental total cost of cirrhosis by etiology, presence, and types of cirrhosis complications, comorbidity, MELD-Na score, and acute kidney injury. Model 1 adjusted for age, sex, race/ethnicity, socioeconomic status, health insurance, comorbidity (Deyo index), depression, and anxiety. Models 2, 3, 6, and 7 were adjusted for age, sex, race/ethnicity, socioeconomic status, dual health insurance, comorbidity (Deyo index), depression, and anxiety. Model 4 was adjusted for age, sex, race/ethnicity, socioeconomic status, dual health insurance, depression, and anxiety. Model 5 was adjusted for age, sex, race/ethnicity, socioeconomic status, dual health insurance, comorbidity (Deyo index), and anxiety. CI, confidence interval; HCV, hepatitis C virus; MELD-Na, Model for End-Stage Liver Disease-Sodium; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis.
The cost of managing patients with cirrhosis exceeded the cost of managing patients with COPD, ranging from $21,675 (95% CI $17,285–26,065) in year 1 to $11,098 (95% CI $6,302–15,893) in year 3. Compared with patients with CHF, the incremental adjusted costs for caring of patients with cirrhosis were $11,789 (95% CI $1,919–21,659) during the first year. The costs of managing patients were similar in the subsequent years (Table 5).

Incremental cost of managing cirrhosis compared with cost of managing COPD or CHF
DISCUSSION
In this large longitudinal study, we found that the incremental cost of care for patients with cirrhosis was substantial ranging from $32,930 to $57,544 per patient per year, and the highest incremental cost incurred in the first year after diagnosis. Most of this cost was accrued for inpatient care. The annual cost of caring for a patient with cirrhosis was higher than the cost of caring for a patient with COPD across all study years. In a recent systematic review, the annual median medical costs for CHF care were estimated at $24,383 per patient, with heart failure–specific hospitalizations driving costs (median $15,879 per patient) (12). In our study, cost of cirrhosis care in the first year exceeded the cost of managing CHF by over $11,000. The cost associated with subsequent years of care was similar for patients with cirrhosis and CHF, showing that the first year after cirrhosis diagnosis may be the period of highest vulnerability. The US Centers for Medicare & Medicaid Services have implemented national value-based programs to incentivize better CHF care (28). Our data support the need to extend such programs to patients with cirrhosis, where the burden of disease is similar, if not greater than that of CHF. Our results are also important because they provide benchmark and comparative cost data for hospitals and payors to implement and test programs specific to patients with cirrhosis.
We also found that cirrhosis costs were highly sensitive to the presence of complications and comorbidities. Patients with AKI, ascites, or hepatic encephalopathy accrued the highest incremental costs. Preventing progression to decompensated cirrhosis, such as through treatment of viral hepatitis and interventions for alcohol abstinence, might offer the highest value by resulting in cost savings, with the greatest benefit in the first year after diagnosis. Furthermore, more than half of patients with cirrhosis had at least 1 additional major comorbid condition that led to additional costs. Multimorbidity was also common, contributed to overall cost of managing patients with cirrhosis, and associated with the highest incremental adjusted cost exceeding $65,000 per patient in the first year alone. Our study also suggests that mental health disorders are associated with substantially higher health care costs among patients with cirrhosis (9–12). Integration of medical and mental health care has been explored in primary care and specialty care (29–31). New models of bundled payment could be developed to support integrated approaches that include the costs of chronic disease and mental health care services (32). In any case, this relationship supports case-mix adjustment in any analysis of cirrhosis costs to control for variability across hospitals due to different distributions of comorbidity in their patient populations.
Our study preceded the COVID-19 pandemic. Several studies show a drop in hospitalization for cirrhosis during the pandemic (33,34). It is plausible that, as the pandemic recedes, there is a rebound in utilization with more patients seeking acute care and requiring hospitalizations resulting from missed or delayed care during the pandemic. This could translate into higher marginal costs of caring for cirrhosis postpandemic and merits an evaluation in future studies.
Our study has limitations. Our analysis represents the cost from the VA perspective. However, given the use of marginal effects that accounted for patterns of health care utilization in control patients without cirrhosis in the VA, our inferences are likely generalizable to non-VA health care systems. Our dataset did not capture care that occurred outside the VA and covered by non-VA health insurance or the VA community care program (VA Choice program), which could result in an underestimation of the true cost of caring for patients with cirrhosis. Only a small proportion of patients in our cohort received liver transplantation (35). Health care costs may be different for patients with greater access to liver transplantation. Our analysis was confined to medical costs, and thus the likely large social costs of cirrhosis (caregiving, absenteeism, etc) are not quantified. Our definition could have underestimated some patients with NASH cirrhosis (such as those who had hypertension or hyperlipidemia).
In conclusion, we found that patients with cirrhosis had substantially higher health care costs than matched controls. The additional economic burden of cirrhosis was mostly related to cirrhosis complications and high inpatient utilization in the first year after diagnosis. Preventing progression to decompensation and programs focused on palliative care (36) have the largest potential for cost saving and could serve as targets for improvement. Multimorbidity was also common in patients with cirrhosis and was associated with total costs. This association supports exploration of bundled payment programs and case-mix adjustment in future evaluations of cirrhosis costs and programs to improve it.
CONFLICTS OF INTEREST
Guarantor of the article: Fasiha Kanwal, MD, MSHS.
Specific author contributions: F.K.: planning and conducting the study, collecting and interpreting data, and drafting the manuscript. She has approved the final draft submitted. R.N.: planning the study, interpreting data, and drafting the manuscript. He has approved the final draft submitted. Y.L.: collecting and interpreting data and drafting the manuscript. She has approved the final draft submitted. J.R.K.: planning and conducting the study, collecting and interpreting data, and drafting the manuscript. She has approved the final draft submitted. R.H.: interpreting data and drafting the manuscript. He has approved the final draft submitted. G.C.: interpreting data and drafting the manuscript. He has approved the final draft submitted. A.R.: interpreting data and drafting the manuscript. He has approved the final draft submitted. A.F.: interpreting data and drafting the manuscript. She has approved the final draft submitted. D.S.: planning the study, collecting data, and drafting the manuscript. She has approved the final draft submitted. Y.C.: collecting and interpreting data and drafting the manuscript. She has approved the final draft submitted. S.M.A.: planning and conducting the study, interpreting data, and drafting the manuscript. He has approved the final draft submitted.
Financial support: None to report.
Potential competing interests: None to report.
Study Highlights
WHAT IS KNOWN
- ✓ Cirrhosis of the liver is a common condition.
- ✓ There are limited longitudinal data on the cost of treating patients with cirrhosis, which limits evaluation of value of care provided to patients.
WHAT IS NEW HERE
- ✓ In this large study of ambulatory patients, we found that patients with cirrhosis had substantially higher health care costs than matched controls.
- ✓ The additional economic burden of cirrhosis was mostly related to cirrhosis complications. Preventing progression to decompensation and hepatocellular cancer has the largest potential for cost saving and could serve as targets for improvement.
- ✓ Multimorbidity also explained a substantial proportion of incremental cost, suggesting that value-based programs in cirrhosis may need case-mix adjustments to control for variability in cost comparisons across hospitals due to different distributions of comorbidity in their patient populations.
REFERENCES





I absolutely love your website.. Excellent colors & theme.
Did you develop this website yourself? Please
reply back as I’m planning to create my own personal blog and would like to learn where you got this from or what
the theme is called. Thank you!