ACG Clinical Guideline: Preventive Care in Inflammatory Bowe… : Official journal of the American College of Gastroenterology
Introduction
The purpose of this article is to review preventive care for the inflammatory bowel disease (IBD) patient. Health maintenance issues include assessment for vaccinations, screening for cervical cancer, melanoma and non-melanoma skin cancer (NMSC), and osteoporosis. Identification of depression and anxiety and smoking cessation in IBD patients will also be reviewed. To accomplish these goals, coordination between the primary care provider, gastroenterology team and other specialists is necessary. Colorectal dysplasia surveillance and management will not be addressed in this review.
As part of this guideline preparation, a literature search was conducted using Ovid MEDLINE from 1946 to 2015, EMBASE 1988 to 2015, and SCOPUS from 1980 to 2015. The major terms were the controlled subject headings in MeSH: IBDs, colitis, ulcerative, and Crohn’s disease. These were translated into the EMTREE controlled vocabulary as enteritis, ulcerative colitis (UC), and Crohn’s disease (CD). Words in the title for these diseases were also included. The balance of the search involved the concepts of interest, including vaccination, immunizations, specific vaccines and diseases, as well as screening, cervical cancer, melanoma, NMSC, smoking, depression, osteoporosis, etc. The results were limited to trials, meta-analyses, systematic reviews, and existing guidelines. In some areas where trials were unavailable cohort studies and reviews were included. Each author performed an updated literature search in 2016 to include more recently published articles.
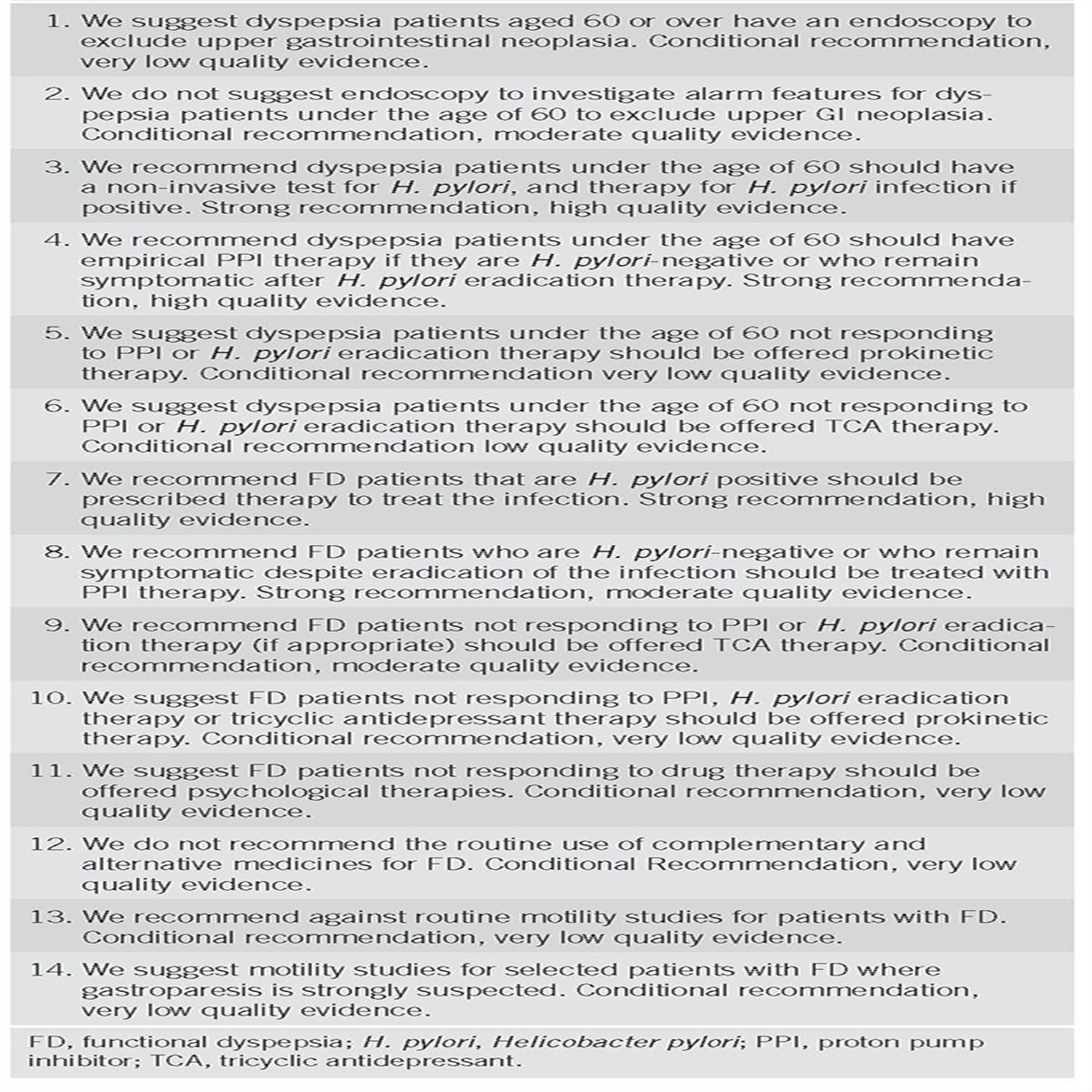
To evaluate the level of evidence and strength of recommendations, we used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system (1). The level of evidence could range from “high” (implying that further research was unlikely to change the authors’ confidence in the estimate of the effect), “moderate” (further research would be likely to have an impact on the confidence in the estimate of effect), “low” (further research would be expected to have an important impact on the confidence in the estimate of the effect and would be likely to change the estimate), or “very low” (any estimate of effect is very uncertain). The strength of a recommendation was graded as “strong” when the desirable effects of an intervention clearly outweigh the undesirable effects and as “conditional” when there is uncertainty about the trade-offs. We preferentially used meta-analyses or systematic reviews when available, followed by clinical trials and retrospective cohort studies. To determine the level of evidence, we entered data from the papers of highest evidence into the GRADE program (accessible at http://www.gradepro.org). The recommendation statements from this guideline are shown in Table 1. Summary statements, when listed, are designed to be descriptive in nature without associated evidence-based ratings.

Preventive health maintenance recommendations
Vaccinations
Recent data suggest that IBD patients do not receive preventive services at the same rate as general medical patients (2). Members of the gastroenterology team are often the only clinicians that a patient with IBD will see. As such, it is incumbent upon gastroenterologists to take a proactive role in the health care needs of their IBD patients (3, 4, 5). It is crucial to clarify with the patient the limits of the specialist’s responsibilities and delegate routine health care issues to the primary care clinician. It is equally important to educate the primary care clinician to the unique health maintenance needs of the IBD patient, especially those on immunomodulators and biologic agents. Although it appears that both primary care clinicians and gastroenterologists are hesitant to take ownership of vaccinations (6, 7, 8), it is reasonable (9) that vaccination recommendations be the responsibility of the treating gastroenterologist, but the actual delivery/administration of these vaccines may be a shared responsibility (10, 11, 12, 13). Communicating specific recommendations to the primary care team in a concise fashion are needed. Consider empowering the patient by giving written recommendations to bring to their primary care physician. Clinicians sharing an electronic medical record should use this platform to send recommendations to the referring clinician.
Patients with IBD are often treated with long-term immune-suppressive therapies and may thus be at increased risk for infections, many of which are preventable with vaccinations (14). In general, adherence to age-appropriate vaccination schedules is recommended, although special considerations exist for patients receiving or initiating immunosuppressive therapies (10, 11, 15). For patients in whom treatment is needed, however, delaying some vaccinations may be necessary to facilitate timely administration of immunosuppressive therapy (10, 11). All adult patients with IBD, regardless of immunosuppression status, should receive non-live vaccines (15, 16) in accordance with national guidelines published by the Centers for Disease Control (CDC), Advisory Committee on Immunization Practices (ACIP) (17, 18) and the Infectious Disease Society of America (IDSA) (10), including trivalent inactivated influenza vaccine, pneumococcal vaccination (PCV13 and PPSV23), hepatitis A, hepatitis B, Haemophilus influenza B, human papilloma virus (HPV), tetanus, and pertussis. Over the last 10 years there has been an increase in the number of cases of measles in the United States, in part related to parents who intentionally have not vaccinated their children (19). A list of inactivated and live vaccines to consider are listed in Tables 2 and 3.

Inactivated vaccine recommendationsa

Live vaccine recommendationsa
Several studies have documented poor uptake of routine vaccinations among patients with IBD (14, 20). In one study of 169 IBD patients seen at an IBD center, of 145 patients on current or previous immunosuppression, only 28% reported regular flu shots and only 9% received the pneumococcal vaccine (14). Common reasons for low rates of vaccination included patient lack of awareness and fear of side effects. In another study of 2076 IBD patients in Spain, only 12% of patients were vaccinated against hepatitis B (20).
In a survey of 108 gastroenterologists in the United States conducted in 2009 there was poor knowledge regarding which vaccines to recommend to the IBD patient (6). In this study, 20–30% would erroneously give live vaccines to immunosuppressed patients while 25–35% would erroneously withhold live vaccines from immunocompetent patients. The majority thought the primary care provider was responsible for determining which vaccinations to give (65%) and for administering the vaccine (83%). A study from Canada demonstrated similar findings (7). A recent study of 178 pediatric gastroenterologists demonstrated practice variation among the gastroenterologists in assessment of immunizations in patients with IBD, including the specific vaccines assessed, and timing and method of assessment (21). Barriers to implementing vaccinations included the inability to coordinate care, access immunization records, and offer vaccines through their medical practice. In this study only 28% believed that primary care practitioners were solely responsible for immunizations. In a survey of family care physicians, only 29% were comfortable making a recommendation for vaccinating their IBD patients (8).
Although all non-live vaccines can be administered to patients regardless of immunosuppression status, certain live vaccines (i.e., herpes zoster vaccine) are recommended for patients on “low-level” but not “high-level” immunosuppression. Patients with low-level immunosuppression include individuals receiving a daily dose of systemic corticosteroids for ≥14 days (prednisone 20 mg/day equivalent and within 3 months of stopping) or receiving alternate-day corticosteroid therapy, and those receiving methotrexate ≤0.4 mg/kg/week and within 3 months of stopping, azathioprine ≤3.0 mg/kg/day, or 6-mercaptopurine ≤1.5 mg/kg/day and within 3 months of stopping. Significant protein calorie malnutrition is also associated with immunosuppression. The IDSA considers patients on anti-tumor necrosis factors (TNFs) to have high-level immunosuppression (10, 11, 15). The package insert for vedolizumab states that patients on this biologic agent may receive non-live vaccines (e.g., influenza vaccine injection, etc) and may receive live vaccines if the benefits outweigh the risks (https://entyviohcp.com/?gclid=CJLM_o6Nj-MoCFZFgfgodybALFw). Patients treated with ustekinumab should not receive live vaccines, and while non-live vaccines can be safely administered, immune responses may be insufficient (https://www.stelarainfo.com/pdf/prescribinginformation.pdf).
One concern raised by clinicians and patients is that vaccination may exacerbate IBD disease activity (12, 16). Several studies of patients with rheumatologic disorders failed to demonstrate that vaccination was associated with an increase in disease activity. There is no convincing evidence that IBD activity will be exacerbated by vaccination. In one study of H1N1 vaccine, 575 patients on immunomodulators or anti-TNFs received vaccine between 11/09 and 3/10 in 14 European countries. The vaccine was well tolerated. Within 4 weeks after vaccination, absence of flare was observed in 377 patients with Crohn’s disease (CD; 96.7%) and 151 with UC (95.6%), which was considered to be consistent with the background rate of relapse (22). Another small study, evaluating the safety and efficacy of the vaccination in patients with IBD on immunomodulator therapy, reported no flares after vaccination (23).
The sections below provide evidence and detail for specific vaccinations in the setting of IBD with and without immunosuppression. Although there are many vaccines to consider, most adults will have already received routine childhood vaccinations. During flu season, influenza vaccination should be prioritized due to the significant morbidity and mortality associated with this common public health hazard especially during epidemic years. Furthermore, pneumococcal vaccination can be safely administered at the same time as influenza vaccination and the two should be considered concurrently when opportunities arise. It is also important for clinicians to be attuned to regional epidemics, such as the pertussis epidemic that appeared in many states between 2010 and 2014 and led to public health advisories for universal Tdap vaccination in many states.
Simple office measures can be easily implemented to improve vaccination rates in clinical practice. In one study, vaccination rates for a high-risk IBD population was significantly improved using a checklist as part of a quality improvement intervention (24). In another study, making influenza and pneumococcal vaccinations available in the gastroenterologists office increased vaccination rates significantly (25). A systematic education of health-care professionals resulted in increased patients’ adherence to vaccination guidelines (26). A checklist reviewing vaccination and general health maintenance recommendations can be found at http://cornerstoneshealth.org/checklist/ and http://www.ccfa.org/science-and-professionals/programs-materials/ccfa-health-maintenance.pdf. With increased attention paid to variability in the type and cost of care delivered to patients, several gastroenterology societies are developing measures to assess quality of care. Systematic efforts should be developed to incorporate quality measures of care in practice (27, 28). Several of the recommendations discussed in this article are included or suggested as quality measures by national or international gastroenterology societies.
Influenza vaccination
Recommendations
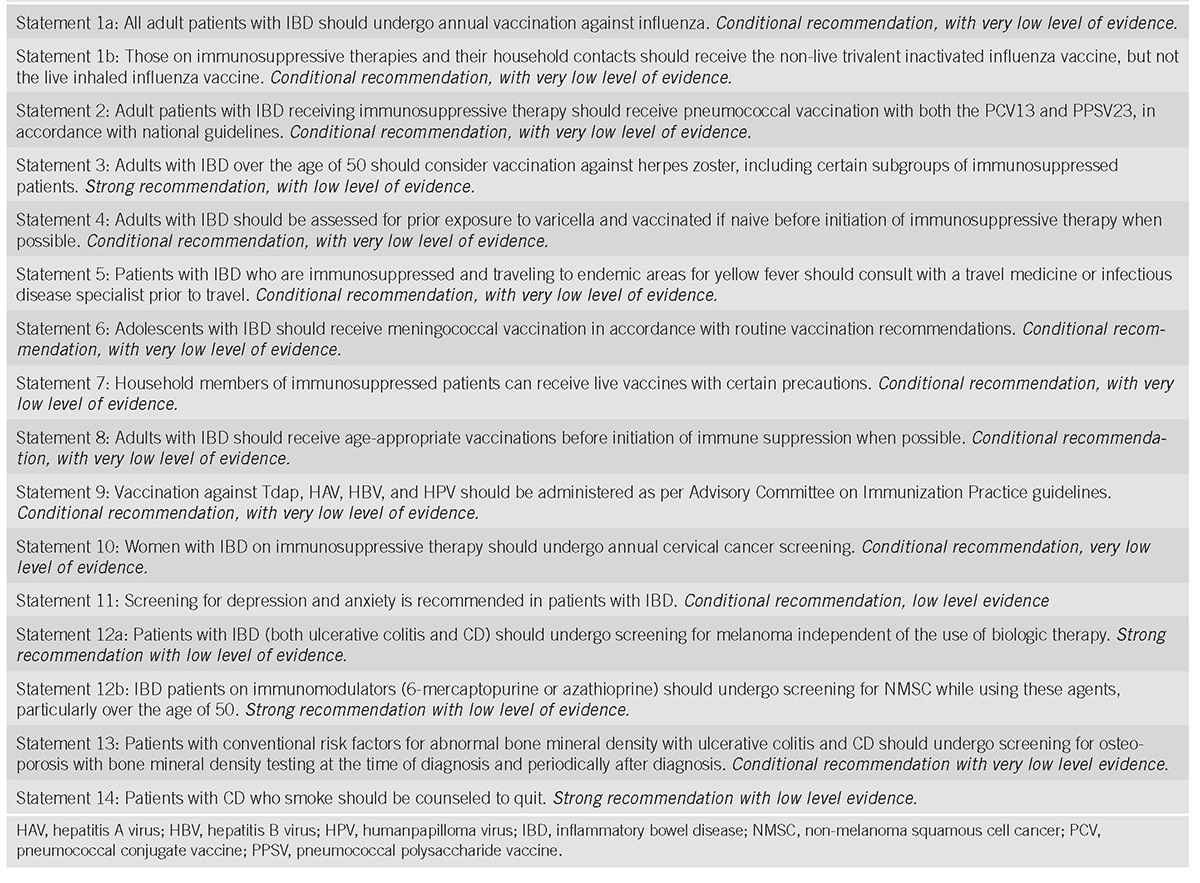
- All adult patients with IBD should undergo annual vaccination against influenza. Conditional recommendation, with very low level of evidence.
- Those on immunosuppressive therapies and their household contacts should receive the non-live trivalent inactivated influenza vaccine, but not the live inhaled influenza vaccine. Conditional recommendation, with very low level of evidence.
Summary of evidence
Patients with IBD are at increased risk for acquiring influenza infection relative to age-matched patients without IBD. This risk is particularly increased when patients are treated with immunosuppressive therapies (29). Furthermore, some patients with IBD who acquire influenza infection are more likely to experience hospitalization and co-infection with pneumonia (30).
Vaccination against influenza has been shown to reduce the risk of infection in several populations, including otherwise healthy adults and children, as well as those with various comorbidities including asthma, cancer, and immunocompromised populations (31).
Influenza vaccination uptake in patients with IBD is suboptimal. Several studies have demonstrated that the most patients with IBD do not receive adequate vaccinations across multiple different healthcare settings (7, 14, 32, 33, 34, 35, 36, 37, 38, 39, 40). This seems to reflect deficiencies in provider knowledge both from gastroenterologists and primary care practitioners (6, 8, 41). However, there appears to be an important role for patient education. In a 2012 survey of 958 patients (median age 45, 73% female, 62% with CD) participating in the Crohn’s and Colitis Foundation of America Patients as Partners cohort, maintaining health (74.1%), importance of prevention (66.1%), and provider recommendation (38%) were the most frequently cited motivations for receiving the influenza vaccine (32).
Several studies have evaluated the safety and efficacy of influenza vaccination among children and adults with IBD and found the vaccines to generally induce appropriate immune responses (42). However, when patients are receiving immunosuppressive therapies with combined thiopurines and anti-TNF agents, serologic responses to vaccines are impaired (22, 23, 43, 44, 45, 46, 47, 48, 49, 50, 51). Nonetheless, even a blunted vaccination response is thought to be of benefit (52) and thus recommendations for influenza vaccination with inactivated vaccine continue to be broadly applicable to all patients, regardless of immunosuppression status (13, 53). The trivalent inactivated vaccine in these studies has been generally well tolerated (42).
Since 2009, universal recommendations for influenza vaccination recommend that all those over the age of 6 months should generally receive influenza vaccination (54). However, because of the theoretical risk of live virus transmission, it is recommended that household contacts of immunosuppressed individuals should receive the trivalent inactivated vaccine and not the the live attenuated influenza vaccine Flumist (Medimmune, Gaithersburg, MD) (55). However, no cases of influenza transmission after live vaccine have been reported among patients with IBD.
Vaccination against influenza among patients with IBD is recommended in several societal guidelines including the American College of Gastroenterology (56), the American Gastroenterology Association (https://www.gastro.org/practice/quality-initiatives/IBD_Measures.pdf), the European Crohn’s and Colitis Organization (57), the North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition (58), and are included as quality improvement measures developed by the American Gastroenterology Association and the Crohn’s and Colitis Foundation of America (56, 58, 59, 60) (http://www.gastro.org/practice/quality-initiatives/IBD_Measures.pdf). Furthermore, widespread public health advisories during flu season suggest a need to prioritize influenza vaccination in general mong patients with IBD, especially among those receiving immunosuppression.
Pneumococcal vaccination
Recommendation
- Adult patients with IBD receiving immunosuppressive therapy should receive pneumococcal vaccination with both the PCV-13 and PPSV23, in accordance with national guidelines. Conditional recommendation, with very low level of evidence.
Summary of evidence
Patients with IBD are at increased risk for pneumonia relative to age-matched patients without IBD (adjusted Cox proportional HR 1.54, 95% confidence interval (CI) 1.49–1.60) (61); this risk is apparent among both CD and UC. This risk appears increased in patients who are being treated with narcotics, corticosteroids, biologic medications, thiopurines, and proton-pump inhibitors relative to patients not receiving these medications (61). Furthermore, patients with IBD hospitalized with pneumonia may be at increased risk of death during hospitalization (62). In a study using the Nationwide Inpatient Sample, no increased risk of pneumococcal pneumonia was identified among individuals with IBD. However risks of pneumonia attributable to influenza virus and Hemophilus influenza were found to be increased among low-income patients with UC and all patients with IBD, respectively (30). In contrast, a recent cohort study of 74,156 IBD patients and 1,482,363 non-IBD controls, the risk of invasive pneumococcal pneumonia was significantly increased both before and after diagnosis of IBD (63). In this study, there was limited impact of the use of IBD medications suggesting that the risk of invasive pneumococcal pneumonia in patients with IBD is related to the underlying altered immune response in these patients. Vaccination against pneumococcal pneumonia is licensed in the United States as the 23-valent pneumococcal polysaccharide vaccine (PPSV23, Pneumovax, Merck & Co., Inc. (Kenilworth, NJ)) and the 13-valent pneumococcal conjugate vaccine (PCV13, Prevnar-13, Pfizer (New York, NY)). Studies in adults with IBD have shown that immune responses to PPSV23 are impaired among patients receiving immunosuppression with thiopurines together with anti-TNF therapy (64, 65). Most studies performed in the literature among patients with IBD and rheumatological conditions including patients treated with anti-TNF therapy suggest that pneumococcal vaccine responses are most influenced by the presence of an immunomodulator (thiopurine or methotrexate) but not monotherapy with anti-TNF (42). PCV13 has been shown to be safe and effective in children with IBD (66).
Vaccination with both PPSV23 and PCV13 is recommended for those receiving immunosuppressive treatment, to maximize the breadth of serotypes covered (i.e., with PPSV23) and ensure optimal protection against the most common and virulent strains (i.e., with PCV13 (10, 11). Thus, children and adults receiving immune suppressive therapies should receive a single dose of PPSV23 followed by a single booster dose 5 years later (10, 11, 17). In addition, a single dose of PCV13 should also be administered either >8 weeks before PPSV23 or >1 year after PPSV23 (10). Pneumococcal vaccination can be safely administered at the same time as influenza vaccination, thus providing an opportunity to educate and target patients appropriate for pneumococcal vaccination during flu season (17).
Herpes zoster vaccination
Recommendation
- Adults with IBD over the age of 50 should consider vaccination against herpes zoster, including certain subgroups of immunosuppressed patients. Strong recommendation, with low level of evidence.
Summary of evidence
Herpes zoster (HZ) commonly is a painful, dermatomal cutaneous eruption that occurs most frequently among older adults and immunocompromised individuals. The disease results from the reactivation of latent varicella-zoster virus (VZV) within dorsal root ganglia (67). In the general population, about one in three persons will develop zoster, or a zoster-related diagnosis, during their lifetime, with an increased incidence with age due to weakening cellular immunity. As many as 10–18% of patients may also develop debilitating post-herpetic neuralgia (68).
Patients with IBD are at increased risk of developing herpes-zoster infections (69, 70). The risk of herpes-zoster is higher in patients with IBD regardless of duration of disease. Gupta performed a retrospective cohort and a nested case–control study using 1988–1997 data from the General Practice Research Database (71). In the cohort study, 7,823 CD and 11,930 UC patients were matched on age, sex, and primary care practice to 79,563 randomly selected controls without CD or UC. In the nested case–control study, 185 CD patients with zoster and 266 UC patients with zoster were matched to 1787 IBD patients without zoster. In the cohort study, the incidence of zoster was higher in patients with CD and UC compared with their matched controls (UC incidence rate ratio (IRR), 1.21; 95% CI, 1.05–1.40; CD IRR, 1.61; 95% CI, 1.35–1.92). In the nested case–control study, receipt of a prescription for corticosteroids (adjusted odds ratio, 1.5; 95% CI, 1.1–2.2) or azathioprine/6-mercaptopurine (adjusted odds ratio, 3.1; 95% CI, 1.7–5.6) were both associated with zoster.
In another large retrospective cohort and nested case–control study using a large administrative database, 50,932 patients with CD, 56,403 patients with UC, and 1,269 with unspecified IBD, were matched to 434,416 individuals without IBD (72). The IBD cohort had an increased zoster risk compared with non-IBD (IRR: 1.68, 95% CI: 1.60–1.76). After adjustment, IBD patients had a higher risk of zoster than non-IBD (HR: 1.49, 95% CI: 1.42–1.57). In the nested case-control multivariate-adjusted analyses, anti-TNF medications (OR: 1.81, 95% CI: 1.48–2.21), corticosteroids (OR: 1.73, 95% CI: 1.51–1.99), and thiopurines (OR: 1.85, 95% CI: 1.61–2.13) were independently associated with zoster. Risk of zoster was highest with combination anti-TNF and thiopurine therapy (OR: 3.29, 95% CI: 2.33–4.65). In addition, herpes zoster also occurs at a younger age in IBD patients (71).
The herpes zoster vaccine (Zostavax, Merck & Co., Inc.) was licensed in 2006 and recommended by the ACIP in 2008 for prevention of herpes zoster (shingles) and its complications among adults aged ≥60 years (68). Zostavax is a live attenuated vaccine. The minimum potency of zoster vaccine is at least 14 times the potency of varicella vaccine. Zoster vaccine is administered subcutaneously as a single dose. It is not recommended to ask patients about history of primary varicella infection or to check serologic titers for varicella immunity before the administration of zoster vaccine. Patients with a history of zoster are eligible to receive the shingles vaccine. The FDA approved the use of Zostavax in 2011 for adults aged 50 through 59 years based on a large study of safety and efficacy in this age group. However the ACIP elected not to recommend vaccination for individuals for 50–59 for concern of loss of vaccine efficacy as patients age which is when their risk of zoster increases (73).
In 2008 the CDC stated that treatment with low-doses of methotrexate (<0.4 mg/kg/week), azathioprine (<3.0 mg/kg/day), or 6-mercaptopurine (<1.5 mg/kg/day) for treatment of rheumatoid arthritis, psoriasis, polymyositis, sarcoidosis, IBD, and other conditions are also not considered sufficiently immunosuppressive to create vaccine safety concerns and are not contraindications for administration of zoster vaccine. Thus it is appropriate to vaccinate IBD patients on low dose immunosuppression as described above. There is no contraindication to vaccinate household members of immunosuppressed individuals with Zostavax, although if the vaccine recipient develops a post-vaccination rash the immunocompromised household contact should maintain contact precautions until the rash has resolved (10, 11).
It is more controversial whether patients on anti-TNF agents can receive the zoster vaccine. At present the Zostavax package insert and CDC guidelines (68) recommend against vaccination if the recipient is immunosuppressed. Interestingly in a large retrospective administrative database cohort study of over 460,000 patients with immune disorders including IBD, there were no cases of zoster in 633 patients on biologic agents in the 42 days after receiving zoster vaccine. Furthermore when these patients were compared with a cohort of individuals not vaccinated, the adjusted hazard ratio for developing zoster for individuals receiving vaccine was 0.61 (95% CI, 0.52–0.71) over a median of 2 years of follow up. Thus the vaccine use was safe and associated with a lower zoster incidence over a median of 2 years of follow-up (74). These data, although retrospective suggest that vaccinating IBD patients on anti-TNF therapy can be considered on a case by case basis after a discussion of the risks and benefits with the patient. A randomized blinded prospective trial on the safety and effectiveness of the live zoster vaccine in anti-TNF users is underway (NCT02538757). In this study vaccine safety and all serious adverse events and non-serious vaccine-strain varicella events within 42 days of vaccination will be assessed as will the clinical effectiveness of the herpes zoster vaccine in reducing longer-term herpes zoster risk over the ensuing 2 years post vaccination. When available, these data will inform clinicians on the safety of vaccinating anti-TNF treated patients with zoster vaccine. An inactive subunit zoster vaccine containing VZV glycoprotein E and an adjuvant was remarkably effective in a study of 15,411 immunocompetent individuals 50 years and older reducing the risk of developing zoster by 97.2% (75, 76). Although not tested in immunosuppressed patients, an inactivated subunit vaccine may be advantageous for immunosuppressed patients with IBD.
Varicella vaccination
Recommendation
- Adults with IBD should be assessed for prior exposure to varicella and vaccinated if naive prior to initiation of immunosuppressive therapy when possible. Conditional recommendation, with very low level of evidence.
Summary of evidence
Varicella or chicken pox is highly contagious (www.cdc.gov/chickenpox/hcp/clinical-overview.html). It can be spread by direct contact with vesicles or through the air when an infected individual coughs. Based on studies of transmission among household members, ˜90% of susceptible close contacts will get varicella after exposure to persons with disease. Before the vaccine was available, ˜4 million people got chickenpox each year in the United States. About 10,600 of those people were hospitalized, and 100–150 died each year.
Patient recall of chicken pox infection is not accurate for determining seropositivity (77, 78). In one study of 163 pediatric patients with newly diagnosed IBD (mean age was 12 years (range 1–19 years, 62% with CD), 66% of the patients related a history of disease or vaccination. However, measurable titers against varicella were found in only 77% of these patients (77). In another study of 121 IBD patients (86% CD, mean age 37±12.8), previous exposure to VZV was reported by 104 patients, and 97/104 (93%) were VZV-immunoglobulin G seropositive. Seventeen patients, all seropositive, reported negative exposure history. The calculated positive and negative predictive values for the reported history of VZV exposure were 93 and 0% respectively (78). These data suggest that IBD patients be tested for varicella exposure and be vaccinated if nonimmune.
Varicella vaccine is a live attenuated vaccine. The ACIP recommends that children who have never had chickenpox should receive 2 doses of the varicella vaccine at 12–15 months of age and a second dose at 4–6 years of age. People 13 years of age and older who have never had chickenpox or received chickenpox vaccine should get two doses at least 28 days apart. As per the CDC (79) varicella immunity can be documented by any of the following options including (i) documentation of age-appropriate vaccination (at least 2 doses); (ii) laboratory (i.e., serological) evidence of immunity; or (iii) a health care provider documented diagnosis of VZV (79). Varicella vaccination is contraindicated 1–3 months before start of biologics and if on one of these agents. The IDSA clinical practice guideline states that administration of varicella vaccine can be considered for nonvaricella-immune patients who are receiving long-term low-dose immunosuppression (10). Interestingly in a small case series of six pediatric patients who received the varicella vaccine while on thiopurines or infliximab, no adverse events were identified (80). There is no contraindication to vaccinate household members of immunosuppressed individuals with varicella vaccine, although if a recipient develops a post-vaccination rash then contact should be avoided until resolution of the rash (10, 11).
Yellow fever vaccination
Recommendation
- Patients with IBD who are immunosuppressed and traveling to endemic areas for yellow fever should consult with a travel medicine or infectious disease specialist before travel. Conditional recommendation, with very low level of evidence.
Summary of evidence
The yellow fever virus is transmitted to people by the bite of an infected mosquito and is found in tropical and subtropical areas in South America and Africa. There is no specific treatment for yellow fever which can be associated with significant morbidity and mortality, and management is based on treatment of symptoms. Steps to prevent yellow fever virus infection include using insect repellent, wearing protective clothing, and getting vaccinated (http://www.cdc.gov/yellowfever/). Certain countries require confirmation of yellow fever vaccination for entry.
It is recommended that all IBD patients and in particular the immunosuppressed IBD patient be evaluated by an infectious disease clinician or at a traveler’s clinic at least 3 months before their departure so that necessary vaccinations be administered (5, 10, 11, 57). Useful resources for patients include the CDC website to learn about the various infectious diseases endemic to their destination (wwwnc.cdc.gov/travel/destinations/list.aspx).
The yellow fever vaccine is a live attenuated vaccine; no alternative inactivated form of the vaccine is available. The CDC recommends that travelers with severe immune compromise be strongly discouraged from travel to destinations that present a true risk for yellow fever (http://www.cdc.gov/yellowfever/healthcareproviders/index.html). These patients should not undergo yellow fever vaccination, as there is a risk of developing a serious adverse event, specifically yellow fever vaccine-associated viscerotropic disease which is a systemic disease associated with multiorgan failure and death. The CDC states that if travel is unavoidable to an area where yellow fever vaccine is recommended and the vaccine is not given, these travelers should be informed of the risk of yellow fever, carefully instructed in methods to avoid mosquito bites, and be provided with a vaccination medical waiver. Even with a medical waiver, the traveler may be faced with quarantine, refusal of entry, or vaccination on site. The CDC states that family members of people with altered immune status, who themselves have no contraindications, can receive yellow fever vaccine.
If the patient requests to stop their immunosuppressive therapy to receive the vaccine, experts feel that the minimal time before the safe administration of the vaccine can be up to 3 months depending on the type of immunosuppressive regimen. The immunosuppressive treatment should not be restarted earlier than 4 weeks after vaccination (81).
Meningococcal vaccination
Recommendation
- Adolescents with IBD should receive meningococcal vaccination in accordance with routine vaccination recommendations. Conditional recommendation, with very low level of evidence.
Summary of evidence
Meningococcal disease is a rare but serious illness and each case may be life-threatening. Teens and young adults 16 through 23 years old are at increased risk. Meningococcal infection can cause sepsis and meningitis resulting in permanent disabilities and rarely death. Meningococcal vaccines are inactivated and can be administered to all IBD patients regardless of immunosuppression. Several different vaccines are available (82). Serogroup A, C, W, and Y meningococcal vaccine is available as a conjugate (MenACWY (Menactra, Menveo)) or a polysaccharide (MPSV4 (Menomune)) vaccine. Serogroup B meningococcal (MenB) vaccine is available as a two-dose series of MenB-4C vaccine (Bexsero) administered at least 1 month apart or a 3-dose series of MenB-FHbp (Trumenba) vaccine administered at 0, 2, and 6 months; the 2 MenB vaccines are not interchangeable, i.e., the same MenB vaccine product must be used for all doses. The reader is referred to the newest recommendations from the ACIP from 2016 (18).
Live vaccinations in household members of immunosuppressed ibd patients
Recommendation
- Household members of immunosuppressed patients can receive live vaccines with certain precautions. Conditional recommendation, with very low level of evidence.
Summary of evidence
Household members of immunocompromised patients can receive all inactive vaccines. A “cocooning” strategy (83) encourages household members of immunocompromised patients be vaccinated to reduce transmission to the immunocompromised patient and has been endorsed by the ACIP and CDC. The IDSA recommends that household members of immunosuppressed individuals can be safely vaccinated based on the most recently published critical review of the literature (10, 11, 83). In parentheses are the strength of the IDSA recommendation and evidence quality.
- Immunocompetent individuals who live in a household with immunocompromised patients can safely receive inactivated vaccines based on the CDC–ACIP’s annually updated recommended vaccination schedules for children and adults (strong, high) or for travel (strong, moderate).
- Individuals who live in a household with immunocompromised patients age ≥6 months should receive influenza vaccine annually (strong, high). They should receive either: (a) Inactivated influenza vaccine (strong, high) or (b) Live attenuated influenza vaccine provided they are healthy, not pregnant, and aged 2–49 years (strong, low).
- Healthy immunocompetent individuals who live in a household with immunocompromised patients should receive the following live vaccines based on the CDC–ACIP annual schedule: combined measles, mumps, and rubella vaccines (strong, moderate); rotavirus vaccine in infants aged 2–7 months (strong, low); varicella vaccine (strong, moderate); and zoster vaccine (strong, moderate).
- Highly immunocompromised patients should avoid handling diapers of infants who have been vaccinated with rotavirus vaccine for 4 weeks after vaccination due to concern for virus transmission (strong, very low).
- Immunocompromised patients should avoid contact with persons who develop skin lesions after receipt of varicella or zoster vaccine until the lesions clear (strong, low).
Vaccinate prior to immunosuppression
Recommendation
- Adults with IBD should receive age-appropriate vaccinations before initiation of immune suppression when possible. Conditional recommendation, with very low level of evidence.
Summary of evidence
Immune response to vaccination in the IBD patient
There are multiple studies that assessed response to vaccination in immunosuppressed IBD patients (42, 50). In general, patients on monotherapy with an immunomodulator have a normal immune response compared with controls or patients on 5ASAs. In patients on monotherapy with anti-TNF, some but not all studies demonstrate a diminished immune response compared with controls or patients on 5ASAs. Finally, in patients receiving both an immunomodulator and anti-TNF agent, there is a diminished immune response to vaccines compared with those on monotherapy with an immunomodulatory, anti-TNF, or 5ASAs. In rheumatologic disorders, a blunted serologic response to vaccination has similarly been established in patients on combination immunosuppression. In a study of normal individuals receiving parenteral hepatitis B vaccine and oral cholera vaccine, vedolizumab did not alter the response to parenterally administered antigens but reduced the response to oral antigens consistent with its purported gut-selective mechanism of action (84).
Finally, it is unclear whether the absence of a robust serological immune response that is seen in healthy individuals is clinically significant or whether the vaccines offer protection to some degree. In one study, vaccinated patients with lupus, rheumatoid arthritis, and Sjogren’s had lower rates of influenza infection and/or total viral infections (85). As the immune response to vaccination is generally blunted by immunosuppression, the IBD patient should ideally be vaccinated soon after diagnosis before the commencement of immunosuppressive therapy where possible, especially given the unpredictable course of the disease and need for future immune suppressive therapy. Treatment of active IBD takes precedent over delay to administer live vaccines. General recommendations from the IDSA with strength of the recommendation and evidence quality noted are as follows but there is some variation in recommendations dependent on the specific live vaccine administered (10, 11):
- Vaccines should be administered before planned immunosuppression if feasible (strong, moderate).
- Live vaccines should be administered ≥4 weeks before immunosuppression (strong, low) and should be avoided within 2 weeks of initiation of immunosuppression (strong, low).
- Inactivated vaccines should be administered ≥2 weeks before immunosuppression (strong, moderate).
Tdap, hepatitis a, hepatitis b and human papilloma virus vaccinations
Recommendation
- Vaccination against Tdap, HAV, HBV, and HPV should be administered as per ACIP guidelines. Conditional recommendation, with very low level of evidence.
Summary of evidence
All adult patients with IBD, regardless of immunosuppression status, should receive non-live vaccines in accordance with national guidelines published by the CDC, ACIP (17) and the IDSA (11), including hepatitis A (HAV), hepatitis B (HBV), Haemophilus influenza B, HPV, tetanus, and pertussis (10, 15, 86, 87).
Given the importance of HBV infection in IBD patients, specific attention should be given to assessing HBV status. Reactivation of hepatitis B infection has been reported in immunosuppressed IBD patients with serious consequences (88). Testing for HBV infection (HBsAg, HBcAb, and HBsAb) and vaccination of the non-immune patient is recommended before starting anti-TNF’s (10, 11, 57). In healthy individuals, protective antibody concentrations after the primary three dose HBV vaccine series is >95% (89). In contrast, studies on HBV vaccination in IBD patients have reported efficacy rates from 33–76% (90). The efficacy of different vaccination strategies against HBV has been reviewed by Marin and colleagues (91). In one study of 148 patients, 41% of those receiving single doses of Engerix-B at 0, 1, and 6 months attained anti-HBs titers>10 IU/l compared with 75% of patients receiving a faster, double-dose protocol (double doses of Engerix-B at 0, 1, and 2 months) (92). Although routine testing of titers in healthy individuals after HBV vaccination is not recommended, immunocompromised patients should have hepatitis B surface antibody levels checked 1–3 months after completion of the vaccination series (10, 11, 57, 93). There is some debate about what titer level represents adequate protection against hepatitis B, with some groups recommending titers above 10 and another above 100 IU/l (89, 94).
Some experts advise that immunocompromised patients have titers checked every 12–24 months to confirm immunity (94). In those patients with waning protective titers, it is reasonable to give a single booster shot, and if titers do not rise appropriately, consider administration of another 3 vaccination series at the regular dose. Prophylaxis regimens for patients at risk for HBV reactivation were recently reviewed (95, 96).
Other health maintenance issues
In addition to vaccination issues, it is important to identify the subgroups of patients with IBD that have an increased risk of developing cervical cancer, NMSC and melanoma. Additionally assessing bone health, screening for depression and recommending smoking cessation in patients with CD are important measures to address when caring for IBD patients.
Screening for cervical cancer
Recommendation
- Women with IBD on immunosuppressive therapy should undergo annual cervical cancer screening. Conditional recommendation, very low level of evidence.
Summary of evidence
Cervical cancer is caused by persistent infection with oncogenic HPV. Known factors associated with an increased risk of cancer include cigarette smoking and a compromised immune system, both of which can be seen in patients with CD. Although vaccination against HPV remains a recommendation for women aged 9–26 years, most females would have been exposed to HPV by the time they are vaccinated so regular screening remains the best approach to protect women from cervical cancer. The American College of Obstetricians and Gynecologists along with the CDC recommend annual screening for women who have a history of chronic immunosuppression (97).
The data regarding an increased risk of cervical dysplasia and cancer from simply having a diagnosis of IBD are conflicting, but there is a consistent trend for the increased risk associated with the use of immunosuppressants. In addition, some data suggests that women with IBD and particularly those on immunosuppressants are screened even less frequently than the every 3 years as recommended for healthy women (98, 99). Data from the PharMetrics Patient-Centric Database from 1996 to 2005 demonstrated that while 70.4% of women with IBD (n=9356) received cervical testing at least once every 3 years, factors associated with reduced testing included Medicaid insurance (OR, 0.28; 95% CI, 0.19–0.41), and immunosuppressant medication use (OR, 0.81; 95% CI, 0.74–0.88); factors in patients at the highest risk for abnormalities (98). Similarly, in a Manitoba province study, 54% of women with IBD received Pap smear screening but having CD, as well as exposure to immunosuppressant medications were independent predictors of lower use of Pap testing (99). The European Crohn’s and Colitis Organization states “given the excess risk demonstrated in various other contexts of immunosuppression, it is currently recommended that all women with IBD, particularly those receiving immunosuppressants, strictly adhere to a screening program of cervical surveillance and undergo vaccination against HPV, when appropriate” (100).
A recently published meta-analysis found sufficient evidence to suggest an increased risk of cervical high-grade dysplasia and cancer in patients with IBD on immunosuppressive medications with an adjusted odds ratio of 1.34 (95% CI, 1.23–1.46) (101). The analysis included eight studies that were varying size and population source but scored high on quality. Heterogeneity was found and was based on study type (case control vs. cohort). The authors concluded based on the results from pooled data of over 77,000 women, increased screening intervals, like those recommended for other chronically immune suppressed women, is indicated.
The most recent study to date is the experience of the nationwide cohort study from Denmark (102). Over 26,000 women with IBD were matched to women from the general population (N=1,508,000). They found that women with CD were screened as often as healthy women but women with UC were screened slightly more often (IRR 1.06; 95% CI, 1.04–1.08). Women with UC had an increased risk of low-grade (IRR 1.15; CI, 1.00–1.32) and high-grade lesions (IRR 1.12; CI, 1.01–1.25) compared with healthy controls. Women with CD had increased risk of low grade (1.26; 95% CI, 1.07–1.48) and high grade (IRR 1.28; 95% CI, 1.13–1.45) lesions as well as well as cervical cancer (IRR 1.53; 95% CI, 1.04–2.27). Interestingly, these investigators also demonstrated a two-way association between IBD and neoplastic lesions as the IRR was higher for both conditions 1–9 years before IBD diagnosis. Also noted was an 8% increased risk for dysplasia for those women with a history of azathioprine use; this effect was not seen for those on steroids or anti-TNF agents.
Screening for depression and anxiety
Recommendation
- Screening for depression and anxiety is recommended in patients with IBD. Conditional recommendation, low level evidence.
Summary of evidence
The etiology of IBD and disease activity following periods of remission is complex, and likely involves an interaction between multiple factors. Psychological stress has been reported by both care givers and patients to exacerbate disease but the published literature is conflicting, in part due to the inherent difficulty in studying this area and diversity of measurement tools used. However, newer studies and animal data suggest that depression and anxiety play a role in disease course. Addressing or at least identifying these issues in patients can be important for disease management and optimizing the chance for good outcomes.
A recent systematic review found that anxiety was present in 19% of IBD patients vs. 9.6% of the background population and depression was found in 21.2 with IBD vs. 13.4% in non-IBD controls. There was just as much depression in those patients with inactive disease as measured by the Hospital Anxiety and Depression Scale as those with active disease (103).
In 2004, Mittermaier et al. studied the impact of depression on relapse of IBD (104). This was a prospective longitudinal study of 60 patients with IBD in remission. Patients were evaluated every 3 months for 18 months with the Beck Depression inventory (BDI), Spielberger Anxiety inventory, IBD Quality of Life Questionnaire (IBDQ), Perceived Stress Questionnaire, and the Rating for IBD Patient Concerns. At baseline, 28% of patients had depression. A higher BDI score at baseline predicted total number of relapse after 12 and 18 months.
The impact of depression was measured in patients receiving infliximab therapy for their active CD. One hundred consecutive patients underwent assessment of clinical and psychological variables at baseline and at 4 weeks after infliximab. The presence of major depression at baseline predicted a lower remission rate, and a significantly decreased time to re-treatment. Depression was found to be an independent determinant of active disease both at baseline and reevaluation (HR 2.27, 1.36–3.79) (105).
In a case–control study of patients with active CD, anxiety and depression were measured in quiescent vs. active disease (106). Anxiety and depression scores were significantly worse in those not being treated aggressively, and treatment with a thiopurine to achieve remission was associated with improved psychiatric survey scores. However, a later study of 139 patients with IBD, IBS, and hepatitis C enrolled in a 1 year observational cohort prospective study of patient outcomes in relation to psychological co-morbidity (107), there was no relationship between depression and anxiety and total number relapses in the IBD group.
In another Canadian study, 101 patients with CD in remission were followed prospectively for up to a year to examine clinical, biological, and psychosocial parameters as predictors of clinical relapse (108). Monthly measurements of psychological distress and perceived stress were measured. The interaction of perceived stress and avoidance coping were predictors of earlier relapse (HR 7.0, 95% CI, 2.3–21.8) in the 37 patients that experienced a relapse. In a recent study of IBD patients in several Boston area hospitals, surgery appeared to increase the risk for depression and anxiety for both UC and CD, with a risk of 16% in CD and 11% in UC within 5 years of surgery (109). A cohort of 75 patients in remission with UC was followed for a year, with endoscopy and long-term perceived stress measured at baseline (110). The Hospital Anxiety and Depression Scale was also used, and acute perceived stress was measured at baseline and then after 1, 3, 6, 9, and 12 months. Short-term stress (HR 10.5, 95% CI, 1.01–11.0) but not long-term stress nor depression was predictive for risk of relapse.
In humans, Mawdsley et al. (111) studied biochemical markers in serum and rectal mucosa in patients with UC in remission vs. controls. A short-term psychological stress was applied to half of the UC patients and the others were controls. In UC patients, stress increased mucosal TNF alpha release by 102%, and reactive oxygen metabolites by 475% as well as reducing rectal mucosal blood flow by 22% compared with UC patients not given stress and healthy controls.
In a review of 12 studies, antidepressants were found to be effective for treating both psychological and somatic symptoms in patients with IBD (112). A small retrospective study in humans demonstrated the role of antidepressants in managing disease activity in humans (113). Twenty-nine IBD patients (14 UC and 15 CD) and matched controls had disease course reviewed the year before and the year after an anti-depressant was started for a mood disorder. Patients had fewer relapses and courses of steroids in the year after starting an antidepressant than the year before with the controls showing no change. In a retrospective study, while taking antidepressants the majority of patients had inactive disease (114).
In a study on patient adherence, 85 IBD patients were psychiatrically assessed for reasons for non-adherence to medical therapy (115). The presence of depression or other psychiatric disorders was found to be significantly associated with non-compliance with medications. However, a more robust study in follow-up was done by Ediger et al. (116) from Manitoba. In a cross-sectional study on adherence to medication, 326 IBD patients completed a multi-item self-report on adherence (Medication Adherence Report Scale), the Health Anxiety Questionnaire and a Brief Symptom Inventory to assess psychological state. Neither the Anxiety Questionnaire nor the Symptom Inventory was found to significantly correlate with adherent behavior.
A randomized trial of psychotherapy and relaxation on the clinical course of CD from the German Prospective Multicenter Psychotherapy Treatment study did not show an effect at 2 years for episode free course (117). However, in a follow-up study of this cohort, they found in multivariate analysis that steroid intake and depression predicted worse disease outcomes. In the high utilizers of health care, a significant drop in healthcare utilization was noted in those treated vs. not for their depression (118).
Although medical treatment of depression may have an effect on disease course, a systematic review of psychological interventions revealed 21 studies with a high risk of bias. Psychotherapy had no effect on emotional status (4 studies, 266 patients), with a standardized mean difference between groups of only 0.03 (95% CI, −0.22–0.27) (119). Educational interventions were ineffective as well −0.08, (95% CI, −0.29–0.12).
Screening for melanoma and non-melanoma skin cancer
Recommendations
- Patients with IBD (both UC and CD) should undergo screening for melanoma independent of the use of biologic therapy. Strong recommendation with low level of evidence.
- IBD patients on immunomodulators (6-mercaptopurine or azathioprine) should undergo screening for non-melanoma squamous cell cancer (NMSC) while using these agents, particularly over the age of 50. Strong recommendation with low level of evidence.
Summary of evidence
Widespread use of anti TNF therapy and immunomodulator therapy has led to the recognition of two malignant complications associated with the use of thiopurines and anti-tumor necrosis factor therapy: NMSC associated with the past or current use of thiopurines and the potential for melanoma in patients with IBD or those exposed to anti-TNF therapy.
It is suggested that all individuals who are initiating immunosuppression therapy for the treatment of IBD should use sunscreen that is protective against UVA and UVB light as well use sun protective clothing. There have been no randomized trials performed in patients with IBD assessing this recommendation; however, early detection, including performing regular skin self-examinations and physician skin examinations has been found to result in melanoma diagnoses at earlier stages, when the disease is most treatable (120, 121). Thus, it is suggested that all IBD patients should follow a program of sun protection and dermatological surveillance, which takes into account their other non-IBD-related risk factors for skin cancer development (122, 123). In addition, education on skin cancer risk and rapid referral for skin abnormalities is appropriate in this patient population.
It is recommended that all patients starting or who are already on immunosuppressive medications should be evaluated by a dermatologist, so that risk assessment according to the individual risk factors and a tailored and case-by-case surveillance strategy is defined for each patient. Although not evidence based, this logical approach has been suggested by some individuals (124). In addition, based on the results from the CESAME study, skin surveillance strategies need to be maintained even after stopping thiopurine therapy; which differs from the recent date of the nationwide VA cohort study.
Epidemiology in IBD patients
A recent meta-analysis (125) demonstrated a cumulative pooled crude incidence rate of melanoma in patients with IBD to be 27.5 cases/100,000 person-years (95% CI, 19.9–37.0). Overall, IBD was associated with a 37% increase in risk of melanoma (12 studies: RR, 1.37; 95% CI, 1.10–1.70) compared with the general population. The risk was increased among patients with CD (seven studies: RR, 1.80; 95% CI, 1.17–2.75) and UC (seven studies: RR, 1.23; 95% CI, 1.01–1.50). The risk of melanoma was higher in studies performed before patients were treated with biologic therapies (studies done before 1998; eight studies: RR, 1.52; 95% CI, 1.02–2.25), but not in studies performed after 1998 (two studies: RR, 1.08; 95% CI, 0.59–1.96). Based on this recent meta-analysis, IBD has been associated with an increased risk of melanoma, independent of the use of a biologic.
Patients with IBD are likely to have the same risk factors as the general population, but in addition have treatment-specific risks. There is no suggestion that IBD itself increases the risk for NMSC. Several earlier studies did suggest an independent risk for NMSC in patients with IBD, but careful evaluation demonstrates that they failed to take into account the patients’ use of antimetabolite therapy. The cumulative data on NMSC risk in patients with IBD highlight that there is an increased risk with the use of immunosuppression, particularly thiopurine use.
In general, the presence of chronic immunosuppression has been linked to an increased risk for the development of squamous cell carcinomas (SCC) and to a lesser degree also basal cell carcinomas (BCC) (126, 127, 128, 129, 130). Most studies regarding NMSC in patients on immunosuppression have been reported in solid organ transplant patients. Little has been published regarding the incidence of NMSC in patients with IBD.
In patients who have had solid organ transplantation, the incidence of SCC is higher as the duration and the level of immunosuppression increases, and it also increases in areas where there are sunny climates (131, 132). Within a period of a decade after transplantation ˜35% of heart transplant recipients will develop a skin cancer. The risk of metachronous lesions in patients with one prior BCC or SCC has been demonstrated to be high in heart transplant patients with 60–70% developing a subsequent SCC within 5 years (128, 133). When cutaneous SCCs develop in patients with transplants who are receiving immunosuppressive therapy the tumors seem to be more aggressive than those patients not receiving immunosuppressive therapy. In general, there is an increased risk of local recurrence, regional and distant metastasis, and mortality compared with other patients (129). This background demonstrating an increased risk of skin cancer in patients who are immunocompromised from transplantation lead to the assessment of the risk for SCCA and BCCA in patients with IBD.
Immunosuppressive agent use in patients with IBD and their risk
There has been concern that immunomodulators and anti-TNF therapy may increase the risk of skin malignancies in patients with IBD. In particular, there is concern that immunomodulators (azathioprine and 6-mercaptopurine) increase the risk of NMSC and also there were some concerns that anti-TNF may accelerate the development of the more aggressive and deadly melanoma. The relationships between methotrexate, natalizumab, vedolizumab, and skin malignancy in IBD have not been adequately studied.
There has not been a suggestion of any escalation of the risk of melanoma in patients receiving thiopurines. Recently, however, a study performed by Long et al. (134) evaluated the risk of melanoma in IBD and in relation to drugs, and verified that the use of anti-TNF for 1 year conferred an almost twofold (OR, 1.88; 95% CI, 1.08–3.29) increased risk for developing this malignancy, even after adjusting for health care utilization and comorbidities. Therefore, this study should alert clinicians to be watchful for the development of skin cancer (melanoma in particular) in patients under anti-TNF monotherapy (134, 135, 136, 137). Further confirmation in large prospective analyses is important to validate these initial observations.
There have been several studies that have highlighted an elevated risk of NMSC in patients with IBD (134, 138, 139, 140, 141, 142, 143, 144, 145, 146). It is recognized that individuals who use antimetabolite therapy with either azathioprine or 6-mercpatopurie whether current or prior use- escalates the risk of NMSC for users.
A recent meta-analysis (which evaluated eight studies involving 60,351 patients provided data on the risk of developing NMSC in patients with IBD on thiopurines) evaluated the aggregate of all published studies to discern the magnitude of the elevation of the risk for patients with IBD on immunomodulators to develop NMSC compared with those who do not use thiopurines. This meta-analysis has shown that the risk of developing NMSC with thiopurine use in patients with IBD is 2.28 (95% CI, 1.50–3.45) and is 1.83 (95% CI, 1.2–2.80) when population-based studies are included. Thus, the risk for NMSC is modest in patients with IBD who use thiopurines and the risk vs. benefit needs to be determined in all patients who use these agents.
In addition, in the CESAME study, investigators have assessed the risk of past use of thiopurines and compared the risk with current users. The increased risk of NMSC in IBD patients who receive thiopurines was increased with a HR of 5.9 (95% CI, 2.1–16.4; P=0.0006) for ongoing treatment and 3.9 (95% CI, 1.3–12.1; P=0.02) for past exposure in the CESAME cohort study (147). When assessing the risk based on patient’s age; these values were 2.59/1,000 and 1.96/1,000 patient-years for the age group of 50–65 years and 4.04/1,000 and 5.70/1,000 patient-years for patients older than 65 years. Among patients who had never received thiopurines, the incidence of NMSC was zero before the age of 50 years, 0.60/1,000 for the ages of 50–65 years, and 0.84/1,000 for those older than 65 years. In light of this, it is recommended to evaluate these patients with periodic skin examination especially in patients over the age of 50 years. Another recent study suggests that the risk for NMSC reverts to the baseline population risk on cessation of the thiopurines (148, 149). This study evaluated 14,527 patients with UC in the analysis, with a median follow-up of 8.1 years. A total of 3,346 (23%) patients used thiopurines for a median duration of 1.6 years. There were a total of 421 NMSC and 45 MSC cases. The adjusted hazard ratios of developing NMSC while on and after stopping thiopurines were 2.1 (P<0.0001) and 0.7 (P=0.07), respectively, as compared with unexposed patients.
It remains uncertain if there is additive or synergistic risk for patients who use combination therapy (anti-TNF therapy and immunomodulator therapy) when compared with monotherapy with either agent alone. Please see Supplementary file 1 for additional background information on skin cancer.
Screening for osteoporosis
Recommendation
- Patients with conventional risk factors for abnormal bone mineral density with UC and CD should undergo screening for osteoporosis with bone mineral density testing at the time of diagnosis and periodically after diagnosis. Conditional recommendation with very low level evidence.
Summary of evidence
It has been recognized that reduced bone mineral density (BMD) and bony fractures are more common in persons with IBD, however, the actual disease burden is not well characterized. Also, the impact of IBD-associated factors and IBD-specific inflammation on bone is not well characterized. It has been estimated that 14–42% of persons with IBD have osteoporosis, though the precise prevalence is unknown, as there are no population-based data with universal case detection (150, 151, 152). Not all persons with IBD are at equivalent risk for developing osteoporosis or developing an osteoporosis-related fracture. There are specific risk factors associated with the development of accelerated bone mineral loss, osteoporosis, and fracture in IBD.
The pathogenesis of bone loss in patients with IBD is complex, multifactorial, and incompletely understood. Patients with IBD have an increased risk for loss of bone mass. The pathophysiology of IBD-related osteoporosis is multifactorial; however, risk factors such as steroid treatment, systemic effects of chronic inflammation, calcium and vitamin D deficiencies, and malnutrition are known to be involved (151, 153, 154).
There have been few population-based cohort studies evaluating the prevalence of metabolic bone disease in IBD and on the specific risk factors for low BMD in IBD. Several studies have implicated the presence of a low BMD in patients with IBD whereas others have not (155, 156, 157, 158). Two population-based European studies revealed that the risk of IBD itself causing major osteoporotic fracture decreased when there was adequate control for recent glucocorticoid use (159, 160).
In the past it had been hypothesized that having IBD is an independent predictor for the development of metabolic bone disease, as a result of the inflammation that was present which occurred independently of concomitant confounding variables such as corticosteroid use, decreased body mass index, and dietary deficiency and/or malabsorption of vitamin D and calcium. Currently, however, there is inadequate data to support the contention that inflammation within the bowel itself is an independent predictor of bone mineral loss in IBD. It has been suggested that the increased risk of fracture seen in previous analyses of IBD patients is likely explained by unadjusted confounders such as low BMI, use of glucocorticoids, or calcium/vitamin D deficiency (156).
Patients with ulcerative status and conventional risk factors for abnormal bone mineral density should undergo screening for osteoporosis. Even after having surgery, UC patients with an ileal pouch anal anastomosis need to be monitored for abnormal BMD with periodic Dual-energy X-ray absorptiometry (DEXA) scanning (161).
If all patients with IBD had BMD assessment initially and then again within a year, this method of practice would be comforting and enable patients and practitioners to see if any alteration over time occurs in BMD. Several investigators have supported this generalized approach given there is a potential for significant morbidity associated when an individual develops this complication (abnormal bone density with the potential for bone fracture).
However, current data does not support this approach to screening because the absolute risk of bone fractures is low. As a consequence of the low prevalence, a more conservative, cost-effective approach that limits screening to all patients with a preexisting fragility fracture, women aged 65 and men aged 70 and older, and those with risk factors that increases the likelihood of detecting low bone mass seems more reasonable.
Thus patients who have IBD should be screened based on established guidelines for the general population. Osteoporosis screening guidelines differ between societies, however, DEXA testing is recommended by the National Osteoporosis Foundation for postmenopausal women aged 65 and men aged 70 and older (162, 163, 164). Also, focused BMD screening is advocated for persons who have conventional risk factors for low BMD, specifically those individuals who have identifiable medical conditions or use of medications that are known to influence BMD. This would thus include a subset of patients with IBD.
A low threshold should be maintained for screening individuals who have used glucocorticoids at any time. BMD measurement (with a DEXA scan) is recommended in all patients starting oral corticosteroid therapy specifically in those who have used oral corticosteroid therapy for longer than 3 consecutive months in a dose ≥7.5 mg/day of prednisone-equivalent in the absence of baseline BMD measurement. Selection of this minimal dose cutoff is as a result of its use in most clinical trials as an inclusion criterion and on epidemiological data showing that the relative risk of vertebral fracture increases from 2.6 with doses of 2.5–7.5 mg/day to 5.2 with doses >7.5 mg/day (165). Please see Supplementary file 2 for additional background information on bone health.
Smoking cessation in patients with crohn’s disease
Recommendation
- Patients with CD who smoke should be counseled to quit. Strong recommendation with low level evidence.
Summary of evidence
As the original report on the effects of smoking on human health by the Surgeon General in January 1964 physicians have recommended smoking cessation to their patients (www.surgeongeneral.gov/initiatives/tobacco/). For CD, there are data to suggest that smoking is associated with (i) development of disease, (ii) disease progression and (iii) poorer medical and surgical outcomes. The first epidemiologic study to document the increased risk of CD associated with smoking came from the UK in 1984, where in a population based cohort of patients who smoked were shown to have more than a threefold risk for developing Crohn’s compared with healthy controls (RR 3.5, 1.8–6.6) (166). Another later population-based case–control study from New Zealand demonstrated a twofold increased risk for cigarette smoking at diagnosis (OR 1.99; 95% CI, 1.48–2.68) (167). Finally, the Oxford Family Planning Association contraceptive study showed that the risk of developing CD in women was more than threefold higher in smokers than nonsmokers (168). In twin studies, Bridger found that in 23 dichotomous twin pairs, the smoker twin had CD in 91% of cases with an OR of 10.5 (95% CI, 2.6–92) and in another more recent study, the smoking twin from discordant pairs demonstrated an OR of 2.9 (95% CI, 1.2–7.1) (169). A meta-analysis by Mahid et al. examined a total of nine studies reporting on smoking and development of CD (170). They found a significant association between current smoking and the development of CD with an OR of 1.76 (95% CI, 1.40–2.22) without significant heterogeneity.
Smoking is also associated with disease progression. Data from 1,420 incident patients between January 1977 and December 2008 found that smoking was associated with a change in disease behavior (P=0.02), development of arthritis/arthropathy (P=0.002), and need for steroids (P=0.06) or thiopurine therapy (P=0.038) (171).
Data from a large Spanish national IBD registry (ENEIDA), including information regarding demographics, clinical characteristics, disease complications, therapeutic interventions, and smoking status demonstrated that in the time-dependent multivariate analysis, smokers were found to have a significantly decreased survival free of stricturing disease (HR 1.5, 1.18–1.90) or perianal complications (HR 1.50; 95% CI, 1.01–1.46), and had a higher risk for requiring thiopurine therapy (HR 1.20; 95% CI, 1.05–1.30) (172).
In the follow-up TABACROHN study, this multi-center cross-sectional study included 1,170 CD patients. Patients were classified as nonsmokers, current smokers, or former smokers according to their present smoking status. Smokers were more frequently under maintenance treatment when compared with nonsmokers. In addition, current smokers presented higher use of biologic drugs compared with nonsmokers. Tobacco exposure and a higher tobacco load were independent predictors of need for maintenance treatment and stenosing phenotype, respectively (173).
In a recent meta-analysis, To et al. (174) found in 33 studies a 56% higher risk of a flare of disease activity and a twofold risk of flare after surgery along with a need for first surgery (OR 1.68; 95% CI, 1.33–2.12) and the need for second surgery (OR 2.17; CI, 1.63–2.89) in smokers.
Smoking also appears to adversely affect response to therapy. Early reports of anti-TNF therapy found that 22% of smokers vs. 74% of nonsmokers responded to episodic use of infliximab (175), and a prospective study of 74 patients given a single dose of infliximab found that at 4 weeks smokers were less likely to have a response (OR 0.22; 95% CI, 0.08–0.41) and a shorter duration of response than non-smokers (176). In a retrospective study, patients with CD who continued to smoke required new courses of steroids and in multivariate analysis, smoking status was the only predictive factor of drug tolerance (177).
In a retrospective study of 83 patients with CD who underwent endoscopic balloon dilation of an intestinal stricture, Gustavsson found among current smokers, 97% underwent another intervention compared with only 55% among never smokers (adjusted HR 2.50; 95% CI, 1.14–5.50). After 5 years, the cumulative probability of a new intervention was 0.81 in smokers compared with 0.52 in never smokers the difference 0.29 (95% CI, 0.07–0.52) (178).
The positive effect of smoking cessation has also been demonstrated. Ryan et al. (179) reported on the effect of smoking cessation on surgical outcomes with a favorable outcome in those quitting less likely to have undergone 1, 2, and 3 re-operations for recurrence at any site and were less likely to have undergone one re-operation for recurrent ileocecal CD than those who continued to smoke.
In a controlled trial of the effect of smoking cessation on CD, repeated counseling to stop smoking, with easy access to a smoking cessation program, was given to 474 consecutive smokers with Crohn’s disease. Patients who stopped smoking for more than 1 year (quitters) were included in a prospective follow-up study, which compared disease course and therapeutic needs with 2 control groups, continuing smokers and nonsmokers, paired for age, gender, disease location, and activity. There were 59 quitters (12%). Predictors of quitting were the physician, previous intestinal surgery, high socioeconomic status, and in women, oral contraceptive use. During a median follow-up of 29 months (1–54 months), the risk of flare-up in quitters did not differ from that in nonsmokers and was less than in continuing smokers (P<0.001). Need for steroids and for introduction or reinforcement of immunosuppressive therapy, respectively, were similar in quitters and nonsmokers and increased in continuing smokers (180).
There are several proposed biologic mechanisms as possible explanations for this association ranging from altered autophagy and consequent epithelial oxidative damage (181), genetics with altered IL23R SNPs (182), dysfunctional mononuclear cells (183), and altered bacterial microbiota profiles in smokers with CD (184).
Conclusions
Patients with IBD often consider their gastroenterologist to be the primary provider of care. Health maintenance issues need to be co-managed by both the gastroenterologist and primary care team. Gastroenterologists need to explicitly inform the primary care provider of the unique needs of the IBD patient, especially those on immunomodulators and biologics or being considered for such therapy. In addition to vaccinations, referral to dermatology, gynecology, psychiatry, and endocrinology may be necessary on a case by case basis. Coordination between the gastroenterology team and other providers is the basis for improving the quality of care that is provided to patients with IBD.
ACKNOWLEDGMENTS
The authors thank Lauren Gerson MD, FACG for developing the GRADE statements for this manuscript.
REFERENCES
Discover more from reviewer4you.com
Subscribe to get the latest posts to your email.