Effectiveness of Helicobacter pylori Treatments According to… : Official journal of the American College of Gastroenterology
INTRODUCTION
Helicobacter pylori infection is the most prevalent infection in the world (1). This infection is the main cause of different diseases such as functional dyspepsia, gastritis, gastroduodenal ulcers, and gastric cancer (2).
H. pylori is a bacterium characterized by the development of resistance to multiple antibiotics. The World Health Organization (WHO) establishes antibiotic resistance as a global health problem (3) and determines H. pylori as one of the bacteria that can potentially cause problems during the eradication treatment because of the growing resistance (4). Antibiotic resistance is one of the main factors that determine the efficacy of the different treatment regimens and somehow hamper the objective of all therapeutical schemes, which is ultimately to achieve an eradication rate equal or higher than 90% (5). Other relevant factors are the adherence and the duration of treatment.
In Europe, resistance to clarithromycin, levofloxacin, and metronidazole in naive patients is generally high, which is above 15% (6). According to Maastricht VI/Florence Consensus, the first-line eradication therapy should be based on the prevalence of local clarithromycin-resistant H. pylori strains (7). A country was defined as one with a high clarithromycin resistance when clarithromycin resistance is equal or higher than 15%–20% (7). Furthermore, antibiotic resistances are markedly increased in patients who have received at least 1 previous treatment, with dual and triple resistances (6).
Based on resistance and the established treatment effectiveness threshold of 90%, most international organizations and guidelines advise abandoning triple therapies that include 2 antibiotics (clarithromycin plus either amoxicillin or metronidazole) and introducing quadruple regimens (either bismuth or non–bismuth-based) (5).
There are few studies evaluating the efficacy of H. pylori treatment in routine clinical practice with known antibiotic sensitivity to H. pylori (i.e, susceptibility-based). Therefore, our objective was to evaluate the effectiveness of first-line and rescue treatments against H. pylori in Europe according to the resistance pattern of the different antibiotics.
METHODS
European Registry on H. pylori Management
The European Registry on H. pylori Management (Hp-EuReg) is an international multicenter prospective noninterventional registry with a collection of information on H. pylori infection management since 2013, which was promoted by the European Helicobacter and Microbiota Study Group (www.helicobacter.org) (8).
The ethics committee of La Princesa University Hospital (Madrid, Spain), which acted as the reference institutional review board, approved the protocol of the Hp-EuReg (8). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a previous approval by the institution’s human research committee. The study was classified by the Spanish Drug and Health Product Agency and registered at ClinicalTrials.gov under the code NCT02328131. Written informed consent was obtained from all participants.
Participants
Data were recorded in an electronic case report form, collected and managed using the web-based application designed to support data capture for research studies (REDCap) (9), and hosted at the Spanish Association of Gastroenterology (www.aegastro.es), a nonprofit scientific and medical society focused on gastroenterology research (10). Data were anonymized. Patients (older than 18 years) with an H. pylori–positive result for culture and antimicrobial susceptibility testing (AST), recruited between January 2013 and December 2021, were included in the analysis. Cases without an antibiogram were excluded. Naive patients were defined as subjects who had never been treated for H. pylori and non-naive those who had previously undergone treatment (one or more eradication treatments).
Data management
After extracting the data and before the statistical analysis, the database was reviewed for inconsistencies and subsequent data cleaning. The data quality review process evaluated whether the study selection criteria had been met and whether data were correctly collected, ensuring the study was conducted according to the highest scientific and ethical standards. Data discordances were resolved by querying the investigators and through group emailing.
Statistical analysis
Variables categorization and definition.
Indications for H. pylori testing were duodenal ulcer, gastric ulcer, uninvestigated or functional dyspepsia, among other conditions. Other indications included a family history of gastric cancer, premalignant gastric lesions such as atrophic chronic gastritis and intestinal metaplasia, anemia of unknown origin, erosive gastroduodenitis, gastric lymphoma, and idiopathic thrombocytopenia.
For H. pylori isolation, gastric biopsy specimens were obtained from the antrum and/or body of the stomach during endoscopic examinations. Cultures were performed on selective plates under microaerobic conditions. AST was performed with E-test strips in most of the centers. Antimicrobial resistance was determined according to the guidelines and criteria of the European Committee of Antibiotic Susceptibility Testing (EUCAST Clinical Breakpoint Table V.9) (https://www.eucast.org/clinical_breakpoints).
Dual resistance was defined as resistance to clarithromycin and metronidazole. Triple resistance was defined as resistance to clarithromycin, metronidazole, and levofloxacin.
Adequate compliance with treatment was defined by having taken at least 90% of the prescribed drugs, accepted as an arbitrary threshold. However, it is known that poorer levels of compliance with therapy are associated with significantly lower levels of H. pylori eradication (11).
All patients included in the study underwent 13C-urea breath test to check the effectiveness of the treatment. The test was performed at least 4 weeks after finishing the treatment.
Only treatment schemes with more than 10 patients treated were considered in the analysis. The treatment schemes used were:
- Sequential; with a proton pump inhibitor (PPI) and amoxicillin 1 g, all twice a day (BID) for 5 days followed by PPI standard dose, clarithromycin 500 mg, and tinidazole 500 mg, all BID for further 5 days, henceforth reported as sequential-PPI + C + A + T.
- Triple with amoxicillin; with a PPI, clarithromycin 500 mg, and amoxicillin 1 g, all BID, henceforth reported as triple-PPI + A + C.
- Triple with metronidazole or tinidazole; with a PPI, amoxicillin 1 g, and tinidazole or metronidazole both 500 mg and all BID, henceforth reported as triple-PPI + A + M/T.
- Bismuth quadruple with the 3-in-1 single capsule (marketed as Pylera); with a PPI and the single capsule 3 tablets 4 times a day; and the aforementioned capsule containing bismuth subcitrate potassium (140 mg), metronidazole (125 mg), and tetracycline (125 mg), henceforth reported as 3-in-1 single capsule.
- Concomitant with metronidazole or tinidazole; with a PPI, amoxicillin 1 g, clarithromycin 500 mg, and metronidazole or tinidazole 500 mg, all BID, henceforth reported as concomitant-PPI + C + A + M/T.
- Quadruple with bismuth subcitrate potassium; with a PPI, amoxicillin 1 g, clarithromycin 500 mg, and bismuth subcitrate potassium 250 mg, all BID, henceforth reported as quadruple-PPI + C + A + B.
- Classic bismuth quadruple; with a PPI, tetracicline 500 mg 4 times a day, metronidazole 500 mg 3 times a day, bismuth subcitrate potassium 120 mg 4 times a day, henceforth reported as quadruple-PPI + Tc + M + B.
- Triple with rifabutin; with a PPI, amoxicillin 1 g BID, and rifabutin 150 mg, BID or once a day, henceforth reported as triple-PPI + A + R.
Data analysis.
The prevalence of bacterial antibiotic resistance was presented as the ratio of the number of the positive cultures resulting in the different antibiotics among the total number of patients where culture and AST had been performed. To compare the treatment schemes, subanalyses by the duration of treatment and adherence to treatment were performed.
Continuous variables were shown as arithmetic mean values and SDs and qualitative variables as percentages and corresponding 95% confidence intervals.
The χ2 test was used to compare categorical variables. The statistical significance was established with a P value ˂ 0.05.
RESULTS
Baseline characteristics
The treatments of 3,970 patients with positive cultures of 27 countries were analyzed. The mean age was 51 years (±15 years), and 62% (2,462) were women. The countries in which most H. pylori cultures were obtained were Italy (2,360; 59.4%), followed by Spain (454; 11.4%), Norway (368; 9.3%), Greece (248; 6.2%), and Slovenia (211; 5.3%).
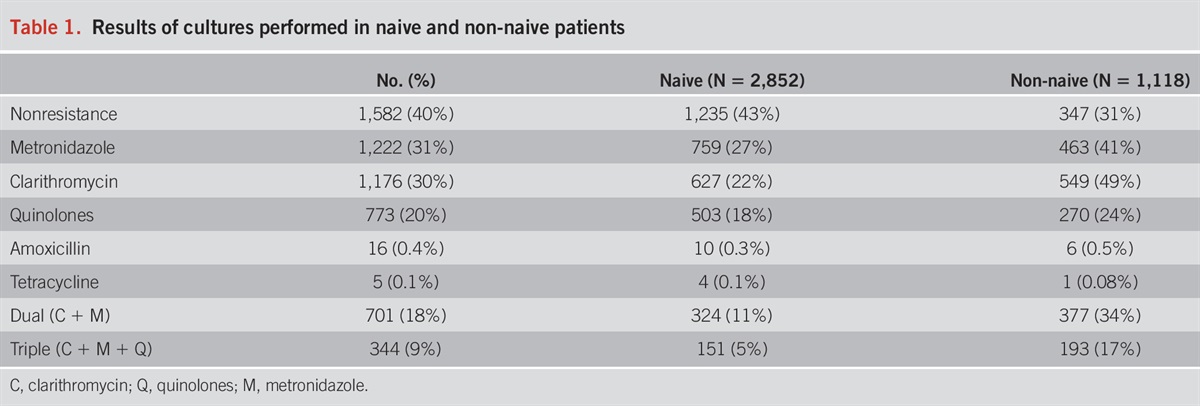
The number of cultures performed in naive and non-naive patients was 2,852 (79%) and 1,118 (31%), respectively. In naive patients, 1,235 (43%) were sensitive to all antibiotics vs 347 (31%) in non-naive patients. The most frequent antibiotic resistance was to metronidazole (31%) and the least frequent to amoxicillin and tetracyclines (less than 1%) (Table 1).

Results of cultures performed in naive and non-naive patients
First-line treatment effectiveness
Patients sensitive to all antibiotics.
The treatments prescribed to 1,235 patients were analyzed. The most commonly used treatment scheme was sequential therapy in 556 (45%) patients, classic triple therapy in 270 (22%), triple therapy with metronidazole in 185 (15%), and concomitant therapy with metronidazole or tinidazole in 71 cases (6%). An eradication rate of at least 90% was achieved in all therapies except in the triple therapy using metronidazole together with amoxicillin, where the cure rate was 88% (Table 2).

Per-protocol effectiveness in naive patients with susceptibility to each of the antibiotics
According to clarithromycin resistance.
In naive patients, the number of patients with resistance to clarithromycin was 22% (627/2,852).
When analyzing the effectiveness of treatments in patients with clarithromycin-sensitive strains, the efficacy of most of the regimens was very high. The highest eradication rate (100%) was reported with the 3-in-1 single capsule (Table 2).
Among the 627 patients with clarithromycin resistance, eradication rates decreased to 75% for instance with triple-PPI + C + A (prescribed in 12 patients). Despite known clarithromycin resistance, the most frequently used regimen was the sequential regimen—including clarithromycin in 50% (311/627) of cases. The treatment scheme with the highest eradication rate was the 3-in-1 single capsule with 93%. The remaining therapies were below 90% effectiveness, except for the quadruple-PPI + C + A + B, reporting 90% eradication rate (Table 3). The concomitant regimen with tinidazole achieved 100% (23/23) eradication vs 74% (20/27) in those treated with metronidazole.

Per-protocol effectiveness in naive patients with resistance to clarithromycin, amoxicillin, and levofloxacin
According to metronidazole resistance.
The rate of resistance to metronidazole in naive patients was 27% (759/2,852). When analyzing the effectiveness of treatments in metronidazole-sensitive patients, independent of other resistances, the efficacy remained similar to that of patients with no resistance. The highest eradication rate was with the 3-in-1 single capsule (100%, 81 patients treated) (Table 2). Despite being sensitive to metronidazole, triple therapy with metronidazole achieved an eradication rate below 90%.
Among the 759 patients with metronidazole resistance, all treatments had eradication rates below 90%, except quadruple therapy with bismuth (94%), treatment with the 3-in-1 single capsule (91%), and triple therapy with levofloxacin (90%), which was used in 49 patients. Most of these patients (39 patients, 80%) had dual resistance to both clarithromycin and metronidazole (Table 3). The concomitant regimen with tinidazole achieved 100% (22/22) eradication vs 73% (16/22) with metronidazole.
According to quinolone resistance.
The levofloxacin resistance rate in naive patients was 18% (503/2,852).
When we analyzed the effectiveness of the treatments in levofloxacin-sensitive patients, independently of other resistances, the success rate remained similar to that of patients with no resistance. The highest eradication rate was with the 3-in-1 single capsule (98%, 80 patients treated) (Table 2). All treatments achieved eradication rates above 90%, except triple therapy with metronidazole (87%). In 69 patients treated with triple therapy with levofloxacin, an eradication rate of 88% was reported.
When we analyzed the 503 patients with levofloxacin resistance, only treatments with quadruple with bismuth (96%), concomitant with tinidazole (100%), and sequential with amoxicillin and tinidazole (93%) achieved eradication rates higher than 90%. The concomitant regimen with tinidazole achieved 100% (22/22) eradication vs 80% (8/10) with metronidazole.
Dual or triple resistance.
Among naive patients, 11% had dual resistance to both clarithromycin and metronidazole. In those cases sensitive to both antibiotics, most treatment schemes achieved eradication rates equal or higher than 90%, being 100% (97 patients treated) in the case of those prescribed with the 3-in-1 single capsule. Triple therapy with metronidazole achieved 87% (197/226) eradication, despite being sensitive to metronidazole.
In patients with dual resistance, triple therapy with levofloxacin achieved 90% (35/39) eradication (see Supplementary Table 1, https://links.lww.com/AJG/D125). The most frequent regimen used was sequential therapy with amoxicillin and tinidazole, with an eradication rate of 85% (157/185), whereas the 3-in-1 single capsule achieved an eradication rate of 86% (24/28).
Triple resistance to clarithromycin, metronidazole, and levofloxacin in naive patients occurred in 5% of the cases (151/2,852). In these cases, the only regimen with more than 15 cases treated was the sequential regimen with amoxicillin and tinidazole, which achieved an eradication rate of 87% (90/103). The next 2 regimens with more cases treated were the 3-in-1 single capsule, with 88% (15/17), and triple with amoxicillin and rifabutin, which achieved 100% eradication (10/10).
Rescue (from second- to sixth-line) treatment effectiveness
Among those non-naive, 49% (549/1,118) of patients were resistant to clarithromycin. Resistance to metronidazole was 41% (463/1,118) and 24% (270/1,118) to quinolones.
Overall, no treatment achieved an eradication rate of 90%. The schemes with the highest eradication rates were the 3-in-1 single capsule with 87% (150/172) and the triple therapy with levofloxacin with 85% (299/352). The triple therapy with rifabutin achieved an eradication rate of 80% (199/249).
Although they were sensitive to clarithromycin, triple therapy with clarithromycin achieved an eradication rate of 76% (see Supplementary Table 2, https://links.lww.com/AJG/D125). The only treatment that achieved eradication rates of 90% with more than 10 patients treated was the 3-in-1 single capsule (90%). In clarithromycin-resistant patients, any of the treatments prescribed to more than 10 patients achieved rates equal or greater than 90% (see Supplementary Table 3, https://links.lww.com/AJG/D125).
In patients sensitive to metronidazole, the only treatment that obtained eradications above 90% was the 3-in-1 single capsule. Triple therapy with metronidazole and levofloxacin achieved eradication rates of 89% and 87%, respectively. In those patients with metronidazole-resistant strains, none of the aforementioned treatments reached 90% cure rates (see Supplementary Table 3, https://links.lww.com/AJG/D125). The best was triple therapy with levofloxacin.
In quinolone-sensitive patients, the 2 treatments that reached optimal (above 90%) effectiveness were triple therapy with metronidazole (92%) and the 3-in-1 single capsule (91%). In levofloxacin-resistant patients, as in the case of metronidazole, none of the treatments achieved 90% cure rates (see Supplementary Table 3, https://links.lww.com/AJG/D125).
Dual or triple resistance.
In non-naive patients, 34% (377/1,118) had dual resistance to clarithromycin and amoxicillin. In those cases, sensitive to both antibiotics, most of the regimens did not achieve eradication rates equal or higher than 90%, despite susceptibility. The only treatment scheme that exceeded 90% was the 3-in-1 single capsule with 93% (50/54) effectiveness (see Supplementary Table 4, https://links.lww.com/AJG/D125). Eradication was significantly lower in non-naive patients than in naive patients (see Supplementary Table 4, https://links.lww.com/AJG/D125).
In non-naive patients with dual resistance, all treatment regimens were below 90% in eradication (see Supplementary Table 1, https://links.lww.com/AJG/D125). By number of cases treated, triple therapy with amoxicillin and rifabutin achieved an eradication rate of 84% (112/134), triple therapy with levofloxacin reached 87% (106/122), and the 3-in-1 single capsule obtained 82% (56/68). The effectiveness was reported lower in non-naive patients than in naive patients (see Supplementary Table 1, https://links.lww.com/AJG/D125).
Triple resistance to clarithromycin, metronidazole, and levofloxacin in non-naive patients occurred in 17% (193/1,118) of cases. In patients sensitive to the 3 antibiotics, the only scheme that reached 90% or more was the 3-in-1 single capsule, with 91% cure rate (73/80). The others schemes with more than 10 cases treated were triple therapy with levofloxacin, with 87% (220/254), triple therapy with amoxicillin and rifabutin, with 70% (39/56), sequential therapy with clarithromycin and tinidazole, with 81% (43/53), triple therapy with amoxicillin and metronidazole, with 89% (33/37), triple therapy with clarithromycin and amoxicillin, with 76% (16/21), and concomitant with metronidazole or tinidazole, with 60% (12/20).
In those non-naive patients with triple resistance, the only regimen with more than 10 cases treated was the triple therapy with amoxicillin and rifabutin, which achieved 86% eradication rate (99/115), and the 3-in-1 single capsule, with 79% (33/42).
DISCUSSION
Clarithromycin and metronidazole are the 2 most commonly used antibiotics in first-line eradication therapy against H. pylori. However, the therapeutical effectiveness will depend on the bacterial resistance to these antibiotics. In recent years, a resistance prevalence of more than 15% has been reported in many geographical areas, which greatly determines the efficacy of the treatments (6,12). In this study, we observed that triple treatments with or without clarithromycin, sequential treatments with clarithromycin and tinidazole, and hybrid treatments with clarithromycin did not reach 90% eradication rate. On the other hand, the schemes concomitant-PPI + C + A + T, quadruple-PPI + C + A + B, and PPI + single capsule achieved eradication rates higher than 90% in those treatment-naive patients with resistant strains to clarithromycin.
Treatment with the single capsule has shown efficacies above 90% in first-line empirical treatment (i.e., without guidance of culture testing) and in those areas where resistance to clarithromycin and metronidazole was above 20%, such is the case of Southern European countries (13,14). Bismuth quadruple treatment with PPI + C + A + B may be also a good option for first-line empirical treatment as suggested by our study, and likewise confirmed in a recent review (15), in which eradication rates of 94% were observed, higher than with concomitant treatment with metronidazole; however, both were above 90%.
A published study of the Hp-EuReg on H. pylori management in which 21,533 patients treated for 5 years were analyzed showed that triple therapy with amoxicillin and clarithromycin during 7 or 14 days was 83% and 87%, respectively, in the per-protocol analysis, independently of the presence or not of bacterial resistance to clarithromycin (16). When susceptible to clarithromycin, the effectiveness of triple therapy was 94%, dropping to 75% in the case of resistance. Similarly, a review study noted that triple therapy in first line including clarithromycin or metronidazole should be avoided when resistances are higher than 15% for clarithromycin (17).
There were fewer studies with triple therapy with levofloxacin in first-line treatment. In general, the results were better than with the classical clarithromycin-based triple therapy (18). In our study, we observed that triple therapy combining amoxicillin with levofloxacin in treatment-naive patients that were resistant to clarithromycin achieved an eradication rate of 88%. This scheme could represent a good option in first-line empirical treatment in those areas with high clarithromycin resistance.
Other regimens that were used in some countries such as in Italy, as the sequential treatment scheme with amoxicillin, clarithromycin, and tinidazole, reported very good results in naive patients sensitive to clarithromycin, but dropped by 8% (from 95% to 87%) when they were resistant to this antibiotic. In our study, sequential treatment tended to be lower than 90% in first-line treatment and lower than in other studies in first-line treatment (19). In other countries (not in Italy), treatment with this scheme had eradication rates higher than 90% (20). In our study, double resistance to both clarithromycin and metronidazole was 11%, which conditioned the effectiveness of this treatment. In studies performed in Italy, double resistance to clarithromycin and metronidazole in naive patients was reported higher than 20%, and the effectiveness of the sequential therapy in such context was only 83% (21,22). On the other hand, in a study comparing the sequential vs the concomitant regimen, the efficacy of the latter was superior (23). The quadruple concomitant regimen with metronidazole or tinidazole, recommended by many clinical guidelines, usually provides very good results in those strains sensitive to clarithromycin (95%), but the effectiveness decreases in those resistant (86%), and thus, its use in first-line empirical therapy is questionable, especially in those regions with high resistance to clarithromycin, similar to those of our study. In this same context, regarding the use of metronidazole or tinidazole, in our study, we observed that the sequential regimen with tinidazole obtained eradication rates of 92% as compared to 80% when metronidazole was used. In a recent review and meta-analysis of randomized controlled trials that compare standard bismuth quadruple therapy vs concomitant therapy for the first-line treatment do not observe differences between both treatments (24). In contrast to our study, Berruti et al (25) performed a study comparing the use of metronidazole 250 mg 4 times a day or tinidazole 500 BID and found no differences between them. Triple therapy with amoxicillin and metronidazole in naive patients sensitive to metronidazole did not reach 90% effectiveness in our cohort, as in other published reviews (25,26). Therefore, metronidazole should not be used in the first-line treatment as part of triple or sequential regimens. One explanation for this result is the fact that there is no good correlation between the susceptibility or resistance of metronidazole in vitro and the efficacy in vivo (27).
In non-naive patients, antibiotic resistance increases considerably (more than 50%) and the efficacy of treatments decreases drastically, all being less than 90% in most studies (6). In our study, the treatments with the highest eradication rates were the 3-in-1 single capsule as well as other combinations that approached 90% (such as the triple therapy with levofloxacin). In the Hp-EuReg, in which 2,448 patients treated as second line were analyzed, triple therapy with levofloxacin, the bismuth-levofloxacin quadruple schemes (PPI-bismuth-levofloxacin-amoxicillin), and the 3-in-1 single capsule were the best treatment options, with eradication rates of 89%, 90%, and 88.5%, respectively (28). In a later study from the same Hp-EuReg, 5,055 patients treated as second line were analyzed, achieving the best eradication rates with either levofloxacin-containing bismuth quadruple therapy (29) or with the 3-in-1 single capsule (13), which was in line with the recommendations of clinical guidelines (5,7). In this sense, to achieve optimal eradication rates in non-naive patients, extending the length of treatment to 14 days and adding bismuth to triple therapy with metronidazole or levofloxacin should be considered.
In our study, we observed that in non-naive patients the in vitro susceptibility of the cultures did not correlate with the effectiveness of the treatments in vivo. Thus, e.g., when non-naive patients were susceptible to clarithromycin, the effectiveness of triple therapy was 76%, whereas the same treatment in naive patients susceptible to clarithromycin obtained 92% effectiveness. The same results occurred in those cases that were susceptible to metronidazole, and the triple therapy with amoxicillin and metronidazole was administered (87%), and again also in those cases that were susceptible to quinolones, the triple therapy with amoxicillin and levofloxacin was prescribed (88%).
The efficacy of treatments depends on antibiotic resistance. In our study, the resistance in both naive and non-naive patients was high to clarithromycin, levofloxacin, and metronidazole. Recently, one of the studies with more cultures performed has been reported (30). In this study, 31,406 gastroduodenal biopsies from patients older than 15 years were plated on selective media, isolating H. pylori in 36.7% (30). Susceptibility testing could be performed in 96.6% (12,399/12,835) of H. pylori isolates. The study was conducted with biopsies collected in Basque Country (Spain) between 2000 and 2021. In naive patients, resistance to any antibiotic analyzed was found in 49.3%, a little lower to our study (57%). In the past 2 years analyzed, the resistance to clarithromycin and levofloxacin has been greater than 15% and 20%, respectively. Resistance to levofloxacin has increased from 7.6% in 2000 to 21.7% in 2021 (30).
The effectiveness of treatment schemes can vary remarkably depending on the area studied because of the variation of resistances. For example, the efficacy of quadruple with bismuth treatment in naive patients in our study was greater than 90% compared with other geographical areas such as Egypt, Iran, and Vietnam where it was only 70% (31).
AST was performed in only 10.5% (2,927/27,776) of naive patients and 15% of non-naive patients. The number of cultures has decreased in these past 10 years. It is important to continue performing cultures or other techniques (polymerase chain reaction – fluorescence in situ hybridization) to determine the tendency of resistance and improve the efficient of treatments (32).
One of the limitations of our study was the lack of a sufficient and homogeneous number of cases in which the study on antibiotic susceptibility was performed (70% of the cultures and treatments came from Italy and Spain), and therefore, there was not a sufficient sample size to study some treatment regimens that are frequently prescribed in Europe. Also, the fact of being an observational study with open inclusion criteria, with the consequent potential higher risk of bias in terms of selection and inclusion of patients, could have hampered the synthesis of the information. To avoid bias, the data selected were defined a priori in the Hp-EuReg protocol to specifically answer the objectives of the study. These data were collected routinely in consultations at platform for Collaborative Research of the Spanish Association of Gastroenterology-Research Electronic Data Capture in a very simple manner, which ultimately avoided potential mistakes. In addition, all participating researchers had previously used this platform or had received training before data entry. Study investigators were selected by the study coordinators based on their experience treating H. pylori infection and their research expertise. Data collection by email or paper was not accepted to avoid increasing errors. Finally, to validate the data entered by the researchers in the database, study monitors systematically checked a random sample of patients from each researcher and/or participating center.
Strengths of this study first included the valuable information from an international multicenter study such as the Hp-EuReg, which includes a large number of evaluated years (9) and countries. Second, the fact that data reflected the daily routine of the clinical practice among European gastroenterologists and not only tertiary hospitals (highly specialized), so in fact allowing for the evaluation of a comprehensive set of data. And the last, the use of the high-quality method to register, store, manage, and monitor the data by using the online platform for Collaborative Research of the Spanish Association of Gastroenterology-Research Electronic Data Capture, allowing the analysis of robust and reliable data.
In summary, in those regions with high H. pylori antibiotic resistance rates, quadruple therapies are recommended both in treatment-naive patients and in those receiving second-line rescue regimens. Bismuth quadruple therapy (including the 3-in-1 single capsule) appeared as the best option in all treatment lines, overcoming clarithromycin and metronidazole resistances. Other first-line alternatives were quadruple therapies with clarithromycin-amoxicillin-tinidazole or clarithromycin-amoxicillin-bismuth. In addition, in second-line therapy, the triple therapy with amoxicillin-levofloxacin might be also an option. Continuous and systematic monitoring of the antibiotic resistance prevalence is necessary to tailor the treatments to the best standards of care in each European region.
CONFLICTS OF INTEREST
Guarantor of the article: Luis Bujanda, MD, PhD.
Specific author contributions: L.B. and O.P.N.: planned and coordinated the study, extracted, analyzed, synthetized, and interpreted the data, wrote the first draft, and approved the submitted manuscript. O.P.N.: Scientific Director and member of the project’s Scientific Committee, planned and coordinated the study, designed, and programmed the electronic case report form, analyzed the data, and approved the submitted manuscript. L.B., J.R., D.S.B., B.T., A.P.-A., M.P., M.C.-F., F.L., M.L., L.R., T.R., J.K., L.J., O.S., A.G., H.S., P.S.P., G.M.B., J.C.M., D.B., L.B., A.T., W.M., M.V., L.V., G.D.F., G.F., E.R., R.M., M.M. and J.P.G.: acted as recruiters, collected or helped interpreting data, critically reviewed the manuscript drafts, and approved the submitted manuscript. L.M., A.C.-C., F.M. and C.O’M.: members of the project’s Scientific Committee, critically reviewed the manuscript drafts, and approved the submitted manuscript. J.P.G.: directed the project and the project’s Scientific Committee, obtained funding, designed the protocol and planned the study, analyzed and interpreted the data, collected patients, critically reviewed the manuscript drafts, and approved the final submitted manuscript.
Financial support: This project was promoted and funded by the European Helicobacter and Microbiota Study Group (EHMSG) and received support from the Spanish Association of Gastroenterology (AEG) and the Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd). The Hp-EuReg was cofunded by the European Union programme HORIZON (grant agreement number 101095359) and supported by the UK Research and Innovation (grant agreement number 10058099). Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the European Union or the Health and Digitial Executive Agency (HaDEA). Neither the European Union nor the granting authority can be held responsible for them. The Hp-EuReg was cofunded by the European Union programme EU4Health (grant agreement number 101101252). This study was funded by Diasorin; however, clinical data were not accessible and the company was not involved in any stage of the Hp-EuReg study (design, data collection, statistical analysis, or manuscript writing). We want to thank Diasorin for their support.
Potential competing interests: J.P.G. has served as a speaker, a consultant, and advisory member for or has received research funding from Mayoly, Allergan, Diasorin, Gebro Pharma, and Richen. O.P.N. has received research funding from Mayoly and Allergan. The remaining authors declare no conflicts of interest.
Informed consent statement: This information is included in the text. “Written informed consent was obtained from all participants.”
Institutional review board statement: The Hp-EuReg protocol was approved by the Ethics Committee of La Princesa University Hospital (Madrid, Spain), which acted as a reference Institutional Review Board (December 20, 2012), and was conducted according to the guidelines of the Declaration of Helsinki, was classified by the Spanish Drug and Health Product Agency, and was prospectively registered at ClinicalTrials.gov under the code NCT02328131.
Study Highlights
WHAT IS KNOWN
WHAT IS NEW HERE
- ✓ In regions where the antibiotic resistance rate of H. pylori is high, eradication treatment with the 3-in-1 single capsule, the quadruple with bismuth and concomitant with tinidazole are the best option in naïve patients.
- ✓ The 3-in-1 single capsule and triple therapy with levofloxacin are the best options for non-naïve patients.
ACKNOWLEDGEMENTS
We want to thank the Spanish Association of Gastroenterology (AEG) for providing the e-CRF service free of charge. The following persons participated in the European Registry on H. pylori Management (Hp-EuReg): Giulia Fiorinni, Ilaria Maria Saracino, Manuel Pabon Carrasco, Alma Keco Huerga, Enrique Alfaro Almajano, Samuel Jesus Martinez Dominguez, Horacio Alonso Galan, Benito Velayos, Carmen Dueñas Sadornil, Jose Maria Botargues Bote, Pedro Luis Gonzalez-Cordero, Miguel Areia, Blas Jose Gomez Rodriguez, Rinaldo Pellicano, Óscar Nuñez, Francesco Franceschi, Sergey Alekseenko, Monica Perona, Rustam Abdulkhakov, Manuel Dominguez-Cajal, Pedro Almela Notari, Judith Gomez Camarero, Manuel Jimenez Moreno, Alicia Algaba, Fernando Bermejo, Jose Maria Botargues Bote, Javier Tejedor Tejada, Elida Oblitas Susanibar, Doron Boltin, Sotirios Georgopoulos, Colm OMorain, Asghar Qasim, Ian Beales, Natalia Bakulina, Galina Fadeenko, Peter Malfertheiner, Rosa Rosania, Tatiana Ilchishina, Pavel Bogomolov, Igor Bakulin, Oleg Zaytsev, Antonietta Gerarda Gravina, Marco Romano, Alfredo Di Leo, Giuseppe Losurdo, Ludmila Grigorieva, Pedro Delgado Guillena, Marinko Marusic, Dragan Jurcic, Natalia Nikolaevna Dekhnich, Eduardo Iyo, Luisa Carmen de la Peña Negro, Natalia Baryshnikova, Natalia Bakanova, Halis Simsek, Cem Simsek, Oleksiy Gridnyev, Miguel Fernandez-Bermejo, Teresa Angueira, Rafael Ruiz- Zorrilla Lopez, Barbara Gomez, Mila Kovacheva-Slavova, Adi Lahat, Javier Alcedo, Ana Campillo, Liya Nikolaevna Belousova, Ramon Pajares Villarroya, Neven Ljubicic, Marko Nikolic, Jesús M González-Santiago, Diego Burgos Santamaría, Anna Pakhomova, Izabela Sekulic-Spasic, Matteo Ghisa, Fabio Farinati, Sabir Irfan Sagdati, Nikola Panic, Frederic Heluwaert, Edurne Amorena, Leticia Moreira, Gloria Fernandez Esparrach, Ekaterina Yuryevna Plotnikova, Michal Kukla, Victor Kamburov, Luis Javier Lamuela Calvo, Ivan Rankovic, Antonio Cuadrado Lavín, Yolanda Arguedas Lazaro, Victor Gonzalez Carrera Agnieszka Dobrowolska, Piotr Eder, Alla Kononova.
REFERENCES
Discover more from reviewer4you.com
Subscribe to get the latest posts to your email.


