


INTRODUCTION
Gastroparesis (GP) is a motility disorder characterized by symptoms and objective documentation of delayed gastric emptying (GE) of solid food without mechanical obstruction, which should be excluded by imaging studies such as upper gastrointestinal (GI) endoscopy or radiology (1,2). The chronic symptoms experienced by patients with GP may be associated with acute exacerbation of symptoms after oral intake of food; the symptoms include postprandial fullness, nausea, vomiting, and upper abdominal pain.
In 2013, the American College of Gastroenterology (ACG) guideline on GP focused on the state of diagnosis and management at the time including assessment and correction of nutritional state, relief of symptoms, improvement of GE, and, in patients with diabetes, glycemic control.
Patient nutritional state should be managed by oral dietary modifications and, if oral intake is not adequate, by enteral nutrition through jejunostomy tube or rarely parenteral nutrition. Medical treatment detailed the use of prokinetic and antiemetic therapies including metoclopramide, short-term use of erythromycin, and gastric electrical stimulation (GES; approved on a humanitarian device exemption), and, in the presence of unmet clinical need, medications used off-label including domperidone, erythromycin (primarily over a short term), and centrally acting antidepressants used as symptom modulators. Second-line approaches include venting gastrostomy or feeding jejunostomy; the latter may be placed directly by percutaneous endoscopic jejunostomy (3). Modifications in percutaneous endoscopic gastrostomy jejunal feeding tubes have reduced likelihood of retrograde displacement of gastrojejunal tubes and reflux of enteral feed back into the duodenal loop and the stomach. These modifications include suture application on the connector and a balloon transgastric jejunal feeding device (4).
Intrapyloric botulinum toxin injection was not effective in 2 randomized, controlled trials (5,6). Partial gastrectomy and pyloroplasty should be used rarely, only in carefully selected patients (7). These procedures have been largely replaced by gastric per-oral endoscopic myotomy (G-POEM), which is discussed in detail in this article.
GP carries a substantial patient burden (8–10), with a negative correlation observed between symptom severity and patient quality of life. The disease also has wider impacts on healthcare burden such as increased hospitalizations and associated direct and indirect economic consequences. Several publications have demonstrated increased morbidity and mortality in patients with GP (11–14). Although GP is known to be associated with use of narcotics in pain syndromes, and opioid agents affect gastric as well as pyloric function resulting in retardation of GE, this was not an objective of the current review and is covered in a separate, recently published article (15). Nevertheless, it is important to emphasize that potent opioids were associated with worse GP (16), and pain associated with GP should not be treated with opioids (including tramadol and tapentadol, which retard orocecal transit and GE, respectively) (17,18). The treatment of pain in GP was not considered in this guideline; there are essentially no clinical trials addressing the treatment of pain in GP. However, the review addresses the use of central neuromodulators and cannabis in GP.
In 2021, members of the European Society of Neurogastroenterology and Motility (ESNM) with expertise in GP and the United European Gastroenterology (UEG) Federation joined forces for developing comprehensive recommendations on GP (19). This involved a Delphi consensus processes, systematic literature reviews, and grading of the strengths of accepted criteria. An initial North American perspective of those recommendations has been recently published (20) with endorsement or further commentary on the recommendations by the ESNM working group, as well as commentary based on the published evidence base.
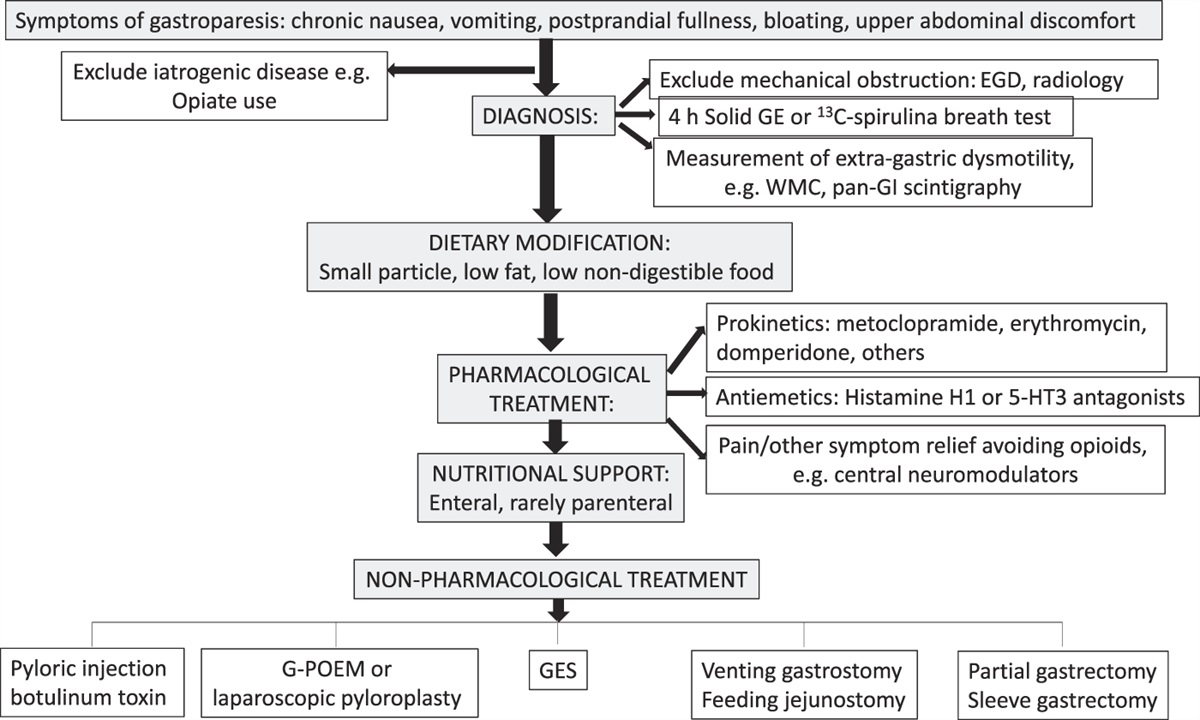
The objective of this new guideline is to document, summarize, and update the evidence and develop recommendations for the clinical management of GP, updating the 2013 ACG guideline on GP (Figure 1) (1). It is necessary to acknowledge the limitations of guideline recommendations on therapies in the absence of Food and Drug Administration (FDA)-approved therapies for GP in the United States and the limitation in duration of prescription to 3 months for the only currently approved medication, metoclopramide.

ACG guidelines are established to support clinical practice and suggest preferable approaches to a typical patient with a particular medical problem based on the currently available published literature. When exercising clinical judgment, particularly when treatments pose significant risks, healthcare providers should incorporate this guideline in addition to patient-specific medical comorbidities, health status, and preferences to arrive at a patient-centered care approach.
METHODS
Key questions
The guideline is framed around several key questions, outlined below. The key questions were developed by the authors and vetted through the ACG leadership. We developed specific questions to address the topics of clinical relevance in the Patient Intervention Comparison and Outcomes (PICO) format (see Supplemental Materials, Supplementary Digital Content 1, https://links.lww.com/AJG/C598). Emphasis has been placed on having practical recommendations that would be helpful for practicing providers in the United States. A broad literature search was conducted to document, by means of detailed tables, information pertaining to the PICO questions, followed by a focused evaluation of the most relevant literature to develop recommendations (Table 1).

Gastroparesis recommendations
Literature search
In February and March 2019, comprehensive literature searches were conducted by 2 health sciences librarians (JP and VMV) in PubMed (MEDLINE), EMBASE, and the Cochrane Library databases. Key concepts from the PICO questions were used to develop search terms and translated to appropriate controlled vocabulary for each database; detailed strategies for each section are provided in Appendix 1 (see Supplementary Digital Content 1, https://links.lww.com/AJG/C598). Results for all searches were filtered for English language publications, and searches regarding therapeutics were further limited to human populations. Searches were updated in May 2021 using the same criteria to capture literature published during the screening and review process. A hand search of references was conducted, and relevant publications identified by content experts were incorporated for analysis.
Screening
Between February 2019 and July 2021, a team of 5 content experts (DA, TA, MC, BK, and LN) screened a total of 1,908 distinct references retrieved by the original and updated searches.
Each reference was screened independently by no fewer than 2 reviewers, with a third reviewer resolving any conflicts. The inclusion criteria were original research studies on the incidence, diagnosis, and treatment of GP in adult populations, predominantly based on observational studies and randomized, controlled trials. Open-label and observational studies of treatment modalities were included in the tables. Exclusion criteria were inclusion in the previous ACG guideline (although, where relevant, these were included in tables for completeness of the literature surveyed), theoretical studies using computational models, animal trials, pediatric populations, and publications without original data analysis.
Although no restriction was placed on publication dates during the retrieval process, emphasis was placed during screening by content experts on studies published after the searches included in the previous guideline, and tables from the 2013 guideline were updated with more recent evidence from the literature. Similarly, searches were not limited by age range within the databases, but any retrieved studies on an exclusively pediatric population were manually excluded during screening. Review articles, correspondence, and other publications without original data were excluded from analysis, although relevant reviews were retained for hand search of their included references.
After screening, a total of 121 references were identified for inclusion and progressed for evidence appraisal in July 2021.
Assessment
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) process (Table 2) (21) was used to assess the quality of evidence for each question, by 2 formally trained GRADE methodologists (RHY and KG) to evaluate the quality of the evidence and strength of the recommendations. The quality of evidence is expressed as high (we are confident in the effect estimate to support a particular recommendation), moderate, low, or very low (we have very little confidence in the effect estimate to support a particular recommendation) based on the risk of bias of the studies, evidence of publication bias, heterogeneity among studies, directness of the evidence, and precision of the estimate of effect. A strength of recommendation is given as either strong (noted as “recommendations,” and meaning that most patients should receive the recommended course of action) or conditional (noted as “suggestions,” and meaning that many patients should have this recommended course of action, but different choices may be appropriate for some patients) based on the quality of evidence, risks vs benefits, feasibility, and costs, taking into account perceived patient and population-based factors. Furthermore, a narrative evidence summary for each section provides important details for the data supporting the statements. The panel have additionally highlighted “key concepts” that were not included in the GRADE assessment. Key concepts are statements to which the GRADE process has not been applied and often include definitions and epidemiological statements rather than diagnostic or management recommendations.

NARRATIVE REVIEW OF EVIDENCE
Risk factors
Recommendation
- In patients with diabetic gastroparesis (DG), optimal glucose control is suggested to reduce the future risk of aggravation of GP (conditional recommendation, low level of evidence).
Optimal glucose control reduces the future risk of aggravation of the GP.
Acute hyperglycemia delays GE in patients with diabetes, and, in the Diabetes Control and Complications Trial and the Epidemiology of Diabetes Interventions and Complications study, delayed GE was associated with GI symptoms and with measures of early and long-term hyperglycemia (22). However, it was unknown whether better glycemic control increases the risk of hypoglycemia or improves hemoglobin A1c levels and GI symptoms in DG.
Continuous subcutaneous insulin infusion and continuous glucose monitoring were assessed in 45 poorly controlled type 1 or 2 patients with diabetes and GP (20). Symptom scores decreased with lower nausea/vomiting, fullness/early satiety, and bloating/distention scores as well as quality-of-life scores, and volumes of liquid nutrient meals tolerated increased at 24 weeks. In conclusion, continuous subcutaneous insulin infusion plus continuous glucose monitoring seems to be safe with minimal risk of hypoglycemic events and associated improvements in glycemic control, GP symptoms, quality of life, and meal tolerance in patients with poorly controlled diabetes and GP. This study supports the safety, feasibility, and potential benefits of improving glycemic control in DG (23). On the other hand, after 6 months of intensive therapy, which led to decreased levels of glycosylated hemoglobin (from mean 10.6% + 0.3% to 9% + 0.4%), GE T1/2 did not change (24). Nevertheless, Izzy et al. (25) documented that HbA1C level is significantly associated with the 4-hour retention value on nuclear GE scan.
Diagnostic testing
After exclusion of mechanical obstruction, diverse tests are available to objectively document the presence of delayed GE. The gold standard is scintigraphic GE (SGE); this section addresses the diverse methods available for diagnosis of GP.
Recommendation
- 2. SGE is the standard test for the evaluation of GP in patients with upper GI symptoms. The suggested method of testing includes appraising the emptying of a solid meal over a duration of 3 hours or greater (strong recommendation, moderate level of evidence).
Optimal duration of GE tests.
It is customary to recommend cessation for 48 hours before the test of medications including opioids, cannabinoids, prokinetics, antiemetics, and neuromodulators with potential impact on the results of the GE test.
Based on a systematic review and meta-analysis (26) of the literature from 2007 to 2017 that included studies evaluating the association between GE (in 92 studies: 26 breath test, 62 scintigraphy, 1 ultrasound, and 3 wireless motility capsule [WMC]) and nausea, vomiting, early satiety/postprandial fullness, abdominal pain, and bloating, 25 studies provided quantitative data for meta-analysis (15 scintigraphy studies enrolling 4,056 participants and 10 breath test studies enrolling 2,231 participants). Meta-regression demonstrated a significant difference between optimal and suboptimal GE test methods when comparing delayed GE with nausea and vomiting. Studies using optimal GE test methodology (that is solid meal and at least 3 hours of data collection) showed significant associations between GE and nausea (odds ratio [OR]: 1.6; 95% confidence interval [CI]: 1.4–1.8), vomiting (OR: 2.0; 95% CI: 1.6–2.7), abdominal pain (OR: 1.5; 95% CI: 1.0–2.2), and early satiety/fullness (OR: 1.8; 95% CI: 1.2–2.6) for patients with upper GI symptoms. Among patients with diabetes, the most significant association with delayed GE was with the symptom of early satiety and fullness but not with nausea and vomiting (26). Therefore, systematic review and meta-analysis supports an association between optimally measured delayed GE and upper GI symptoms. It is worth noting that scintigraphic assessment should be ideally performed up to 4 hours unless it is documented that more than 90% of the solid meal has emptied at 3 hours (27).
Potential confounding between GP and functional dyspepsia
There is increasing attention (28) to the possibility that GP and functional dyspepsia (FD) may be on a spectrum of gastric dysfunction. Despite generally unaltered symptoms over time, 42% of patients initially diagnosed with GP, and 37% of those diagnosed with FD were reclassified based on presence or absence of GE delay on repeat SGE (28). Degree of impairment of GE may vary over time in patients whose symptoms are generally unaltered over the same time. However, it is also conceivable that part of the overlap of the syndromes reflects the cutoff value of 10% retention at 4 hours that is applied to identify patients with delayed GE based on the ingestion of a 255-kcal, 2% fat Egg Beaters meal. Further studies are required to appraise the optimal meal composition and cutoff to define normality to address the reported significant overlap between GP and FD, which may be confounded by the low calorie and fat content of the meal and the use of >10% retention at 4 hours to define delayed GE. It has been emphasized that the distinction between the 2 diagnoses is relevant because of the better prognosis of FD in contrast to the persistence of GP (28).
Diagnosis of GP using scintigraphy
Recommendation
- 3. Radiopaque markers (ROM) testing is not suggested for the diagnostic evaluation of GP in patients with upper GI symptoms (conditional recommendation, very low level of evidence).
Compared with ROM.
There is evidence that GE is accelerated similarly by rectal or oral cisapride when measured by scintigraphy and by ROM (29,30). Several lines of evidence (31,32) suggest that scintigraphy, when compared with ROM, is more accurate in assessing the emptying of the digestible solid food from the stomach. For example, Olausson et al. (32) documented sensitivity and specificity of the ROM test were 34% and 97%, respectively, and in contrast to results from scintigraphy, which correlate with GI symptom severity, results from the ROM test did not. Given that scintigraphy is the gold standard, it is not possible to assess sensitivity and specificity of ROM; however, it is important to acknowledge that the intersubject coefficients of variation (COVinter) for SGE T1/2 were similar in males and females (total 319 healthy controls), overall 24.5% (M 26.0%, F 22.5%), and COVinter for GE at 4 hours was 9.6%. The intra-individual coefficient of variation (COVintra) in 47 healthy controls for T1/2 and GE at 4 hours were 23.8% and 12.6% (33). Similarly, the mean absolute differences in 60 patients with upper GI symptoms undergoing repeat GE studies by scintigraphy an average of 15 days apart were 25 min for GE T1/2 and 7% at 1 hours, 9% at 2 hours, and 7% at 4 hours (34).
Recommendation
- 4. WMC testing may be an alternative to the SGE assessment for the evaluation of GP in patients with upper GI symptoms (conditional recommendation, low quality of evidence).
Compared with wireless motility capsule (WMC).
The results from measurements by SGE and WMC differ. Overall agreement in results between the 2 methods was 75.7% (kappa = 0.42). In subjects without diabetes, the WMC detected a higher proportion of subjects with delayed GE (33.3%) than SGE (17.1%) (P < 0.001); by contrast, a higher proportion of subjects with diabetes had delayed GE detected by SGE (41.7%) than by WMC (17.1%) (P = 0.002). Severe delays in GE were observed in a higher proportion of subjects by WMC (13.8%) than by SGE (6.9%) (P = 0.02). Rapid GE was detected in a higher proportion of subjects by SGE (13.8%) than by WMC (3.3%) (P < 0.001) (35,36). Research supports WMC testing as an alternative test to SGE for the evaluation of GP in patients with upper GI symptoms, and one advantage is that it provides a measure of gastric contractile amplitude, and this can correspond to the timing of capsule emptying documented by the change in pH measured as the capsule traverses the pylorus.
These features underscore the differences in emptying of a solid meal that could be homogenized in the stomach from the emptying of a solid nondigestible capsule, which is greater than 1.5 cm in length and which typically empties from the stomach with the re-establishment of the interdigestive migrating motor complex after the emptying of a meal (37); the capsule is able to provide information about the amplitude of pressure activity in the stomach and small bowel, which may be relevant, e.g., to identify myopathic diseases of the gut or severe antral hypomotility or disorders of motility affecting other regions of the gut such as the small bowel or colon (38). However, overall GP symptoms and nausea/vomiting, early satiety/fullness, bloating/distention, and upper abdominal pain subscores showed no relation to WMC transit (38).
Transit delays beyond the stomach were found in 45.6% of patients with suspected GP who underwent WMC testing: 22.8% small bowel, 31.5% colonic, and 5.4% global (35). Such extragastric dysmotility may be considered in patients with symptoms of GP; indeed, up to 64.7% of patients with symptoms of GP have been found to have slow transit constipation by ROM study (39), and, among 149 patients evaluated at a single tertiary referral center, 77 (52%) had rectal evacuation disorders, and 21 patients (15%) with delayed colonic transit associated with slow ascending colon emptying halftime in 9 and delayed colonic transit because of evacuation disorder in 12 patients (40). The WMC, as with pan-GI scintigraphy, provides opportunity to appraise motor function through the entire GI tract (38,41), which may be indicated in patients with GI symptoms.
Compared with intragastric food identified on upper GI endoscopy.
Retained gastric food (RGF) is frequently identified during esophagogastroduodenoscopy; however, this should not be deemed to be diagnostic of GP. In a retrospective study of 85,116 esophagogastroduodenoscopies, 2991 patients without structural abnormalities had undergone SGE using a standard 320-kcal 30% fat egg meal. Overall, the positive predictive value of RGF for delayed GE was 55%. However, the positive predictive value varied from 32% in patients without risk factors to 79% in patients with type 1 diabetes. Opioids, cardiovascular medications, and acid suppressants were associated with RGF (42). Therefore, the presence of RGF should not be assumed to be diagnostic of GP, and confounding by medications should be excluded in such patients.
Diagnosis of GP using a stable isotope breath test and comparison with scintigraphy
Recommendation
- 5. Stable isotope (13C-spirulina) breath test is a reliable test for the evaluation of GP in patients with upper GI symptoms (conditional recommendation, low quality of evidence).
The stable isotope GE breath test using 13-carbon spirulina has been validated in simultaneous measurements performed with the gold standard scintigraphy and a solid test meal. This has been validated both in patients with upper GI symptoms and healthy controls as well as in pharmacologically induced slowing or acceleration of GE (43,44). Although the kappa statistic is not provided, a validation study of 38 healthy volunteers and 129 patients with clinically suspected delayed GE showed that, at 80% specificity, the 45- and 180-minute samples combined were 93% sensitive to identify accelerated GE, and 150- and 180-minute combined were 89% sensitive for delayed GE (43). The test is also approved for use in children.
Additional value of gastric function tests that do not measure emptying, including electrogastrography
There are the 3 types of cutaneous electrogastrography (EGG): (1) single channel, (2) low resolution, and (3) high resolution. They all measure different aspects of gastric electrical activity. In addition, both mucosal and serosal electrical measurements of EGG are also performed. Single-channel cutaneous EGG measures only frequency; low-resolution EGG measures frequency and amplitude and some measures of propagation; high-resolution EGG measures frequency, amplitude, and more precise measures of propagation such as initiation and conduction of gastric electrical signals. The prevalence of 3 cycles per minute (cpm) electrical control activity measured by single-channel EEG was more prevalent in patients with gastric outlet obstruction compared with patients with idiopathic gastroparesis (IG) or healthy controls (45). High-amplitude and excessively regular 3 cpm EGG patterns were identified in gastric outlet obstruction, whereas high-amplitude and excessively regular 3 cpm EGG patterns differentiated IG and healthy controls and were more likely in those with delayed GE (45,46) and in patients with cyclical vomiting and diabetic gastropathy (47) including uremic diabetics and children with diabetes (48,49). In another study, patients with depleted interstitial cells of Cajal (50) had significantly more tachygastria and significantly greater total symptom scores compared with those patients whose gastric full-thickness biopsies showed less interstitial cells of Cajal depletion.
Using high-resolution electrical mapping (256 electrodes; 36 cm2) (51), it was shown that 9 patients with chronic unexplained nausea and vomiting had slow-wave dysrhythmias, with only 1 of 9 controls showing these dysrhythmias. Dysrhythmias included abnormalities of initiation (stable ectopic pacemakers and unstable focal activities) and conduction (retrograde propagation, wavefront collisions, conduction blocks, and re-entry) across slow, normal, or fast frequencies; dysrhythmias also showed velocity anisotropy (mean, 3.3 mm/s longitudinal vs 7.6 mm/s circumferential; P < 0.01). Such high-resolution, spatial mapping is recommended, especially because of the evidence that abnormalities of slow-wave initiation aberrant conduction and low-amplitude activity in GP often occur at normal frequency, which could be missed by tests that lack spatial resolution (52).
In summary, studies suggest a complimentary role of spatial mapping EGG for identification of the pathophysiologic mechanism of gastric function (53). However, at this time, it is unclear that the information is clinically meaningful. Ongoing research of high-resolution EGG should help clarify its clinical role, including its role in patients with FD.
Other tests for GP based on full-thickness biopsies
The evidence regarding changes at the level of the stomach as identified in histological and molecular studies performed on biopsies taken from patients with GP is detailed in the Supplement. Similar to the ESNM Consensus Statement (19), we do not recommend the routine use of full-thickness biopsies. Full-thickness biopsies should be reserved for research purposes to help better understand the causes of GP, identify biomarkers, guide therapy, and predict outcomes.
MANAGEMENT OF GP
Small particle diet and nutrition interventions
Recommendation
- 6. Dietary management of GP should include a small particle diet to increase likelihood of symptom relief and enhance GE (conditional recommendation, low quality of evidence).
Avoidant/restrictive food intake disorder symptoms are frequent in patients with GP (54), and the ESNM guidelines recommend that eating disorders must be considered in patients with GP (19).
After the pioneering randomized, controlled trial by Olausson et al. (55) demonstrated efficacy of small particle diet compared with normal diet for relief of symptoms, improving GE and enhancing glycemic control (56) in patients with diabetes, a systematic review (57) of all study types evaluated current evidence-based nutrition interventions involving a total of 15 studies and of 524 subjects, using a stepwise process, progressing from oral nutrition to jejunal nutrition and lastly to parenteral nutrition. Small particle, low-fat diets were significantly better tolerated than the converse, with jejunal nutrition before consuming oral food significantly improving oral intake and motility. In more progressive cases, percutaneous endoscopic gastrostomy with jejunal extension nutrition had lower reported symptoms than other enteral routes. Exclusive long-term parenteral nutrition is a feasible option for advanced cases, with a 68% survival rate at 15-year duration, although oral intake plus parenteral nutrition is associated with higher survival rates. The primary role of maintaining or reinstating oral intake was recommended to reduce morbidity and mortality risk.
Pharmacologic agent use in GP
Recommendations
- 7. In patients with idiopathic and DG, pharmacologic treatment should be considered to improve GE and GP symptoms, considering benefits and risks of treatment (conditional recommendation, low quality of evidence).
- 8. In patients with GP, we suggest treatment with metoclopramide over no treatment for management of refractory symptoms (conditional recommendation, low quality of evidence).
- 9. In patients with GP where domperidone is approved, we suggest use of domperidone for symptom management (conditional recommendation, low quality of evidence).
- 10. In patients with GP, we suggest use of 5-HT4 agonists over no treatment to improve GE (conditional recommendation, low quality of evidence).
The 2 medications with the largest number of individual clinical trials for GP are metoclopramide and domperidone.
Metoclopramide is the only US FDA-approved medication for the treatment of GP. The FDA placed a Black Box warning on metoclopramide because of the risk of side effects, including tardive dyskinesia. The efficacy of metoclopramide in the treatment of DG has been assessed in studies that are summarized in Table 3 (58–68), which include newer trials involving the intranasal formulation of metoclopramide. The most common adverse effects of metoclopramide nasal spray were dysgeusia (bad, metallic, or bitter taste), headache, and fatigue.

Trials of metoclopramide for gastroparesis
Regulatory authorities issued restrictions and recommendations regarding long-term use of metoclopramide at oral doses exceeding 10 mg 3–4 times daily because of the risk of development of tardive dyskinesia; the restrictions include use for <12 weeks and age <65 years. Studies in the past decade have addressed the risk of tardive dyskinesia in contrast to reversible involuntary movements on treatment with metoclopramide. First, the relative risk (69) of tardive dyskinesia in metoclopramide users in a VA medical center was not significantly greater than in nonuser controls (relative risk (RR): 1.67; 95% CI: 0.93–2.97). Second, it was estimated that the risk of tardive dyskinesia from metoclopramide use is likely to be <1% (70). The most comprehensive assessment (71) showed that the risk of tardive dyskinesia from metoclopramide is in the range of 0.1% per 1,000 patient years, below a previously estimated 1%–10% risk suggested in treatment guidelines by regulatory authorities. High-risk groups are elderly women, diabetics, patients with liver or kidney failure, and patients with concomitant antipsychotic drug therapy, which reduces the threshold for neurological complications.
The FDA package insert on metoclopramide specifies that restlessness, drowsiness, fatigue, and lassitude occurred in approximately 10% of patients who received 10 mg 4 times daily. No other quantitative data are provided in the FDA-approved insert on the prevalence of other, reversible central nervous system disorders with metoclopramide. One study (72) that documented the epidemiology of extrapyramidal reactions to metoclopramide was studied by examining reports in the Adverse Reactions Register of the Committee on the Safety of Medicines in the United Kingdom in the period 1967–1982. Of an estimated 15.9 million prescriptions, there were 479 reports of extrapyramidal reactions (455 of dystonia-dyskinesia, 20 of parkinsonism, and 4 of tardive dyskinesia). A more recent study of metoclopramide adverse events in the FDA Adverse Event Reporting System for the period 2004–2010 yielded reports of 4,784 neurological reactions and 944 reports were for tardive dyskinesia; the total number of prescriptions was almost 40.5 million (73). These data suggest that 0.1% of prescriptions are associated with nontardive dyskinesia neurological symptoms, which seem to be low estimates and may reflect the fact that medication cessation with reversal of the neurological symptoms may not be reported to regulatory agencies.
Domperidone is available for treatment of GP under a special program administered by the FDA. Table 4 provides a summary of clinical trials with domperidone (63,74–85). Domperidone has been tested in studies that involved patients with IG, DG, or postsurgical GP (PSG), and it has been associated with symptom improvement manifested as lower overall scores or reduction in frequency and intensity of symptoms of GP. Four studies have also documented acceleration of GE compared with control or baseline.

Summary of clinical trials with domperidone
Table 5 summarizes efficacy of other prokinetic agents (5-HT4 and ghrelin receptor agonists) on symptoms or GE (64,86–99). As a group of medications, prokinetics have the most substantive clinical trials, and overall evidence suggests that they provide symptomatic benefit. For all the medications, the recommendation is conditional for use of treatment over no treatment to improve GE. The methodological assessment for the 5-HT4 agonists concluded that there were inconsistent data for symptom improvement.

Summary of efficacy of other prokinetic agents (5-HT4 and ghrelin receptor agonists) on symptoms or GE

Efficacy of antiemetics and central neuromodulators in GP
Another class of agents is the motilin agonists, which are used in the treatment of GP in adults and children. These medications include erythromycin, clarithromycin, and azithromycin. These medications are generally used in the short term (1–4 weeks) because of development of tachyphylaxis to motilides (100). Based on a systematic review and network meta-analysis of 33 studies and data on 22.6 million subjects, macrolide use was not associated with the risk of arrhythmia or cardiovascular mortality (101).
Antiemetics and central neuromodulators in GP
Recommendations
- 11. In patients with GP, use of antiemetic agents is suggested for improved symptom control; however, these medications do not improve GE (conditional recommendation, low quality of evidence).
- 12. Central neuromodulators are not recommended for management of GP (strong recommendation, moderate quality of evidence).
- 13. Current data do NOT support the use of ghrelin agonists for management of GP (strong recommendation, moderate quality of evidence).
- 14. Current data do NOT support the use of haloperidol for treatment of GP (conditional recommendation, low quality of evidence).
Table 6 summarizes efficacy of antiemetics and central neuromodulators in GP (102–108). These are therapies commonly used for symptom relief in GP. The central neuromodulator studied with the highest level of evidence was the tricyclic antidepressant, nortriptyline, in IG (104). In this randomized, placebo-controlled trial, nortriptyline was no better than placebo in relieving global symptoms of GP, but some improvement in abdominal pain was noted. In a study of amitriptyline, 50 mg/d, there was no retardation of GE in patients with FD (109). Further randomized controlled trials (RCTs) are needed to determine the efficacy of other central neuromodulators. Although there are no formal randomized trials, experience with use of haloperidol in emergency department treatment of patients presenting with GP has led to reduced need for morphine treatment and admission to hospitals (110), rather than documenting effect on GP symptoms
Other drug therapies for GP
A recent study has targeted previously described impaired nitric oxide metabolism and an abnormal tetrahydrobiopterin (BH-4) pathway in GP patients with diabetes mellitus. This phase II study needs confirmation in other larger controlled studies (111).
A number of other medications are being developed for treatment of GP. These include 5-HT4 receptor agonists (prucalopride, felcisetrag, and velusetrag) and dopamine D2/D3 receptor antagonists, and the therapeutic trials of these medications are included in Table 5.
Use of pharmacotherapy to reduce the future aggravation of GP
Based on a referral center experience, predictors of responsiveness to pharmacotherapy (112) were identified. A good response to pharmacological agents can be expected in the viral and dyspeptic subgroups of idiopathics, Parkinson disease, and the majority of diabetics; whereas a poorer outcome to prokinetics can be expected in postvagotomy patients, those with connective tissue disease, a subgroup of diabetics (e.g., with evidence of vagal neuropathy), and the subset of IG dominated by abdominal pain and history of physical and sexual abuse (112). The comprehensive NIH GP Consortium database of 748 patients (85) showed 181 (24%) on domperidone and 567 not receiving domperidone; 63% had IG. Compared with patients not receiving domperidone, those patients who were receiving domperidone (median time on domperidone after initiation of 32 weeks, 95% CI: 25–35 weeks) experienced moderate but significantly more improvement in GP outcome measures of the Gastroparesis Cardinal Symptom Index (GCSI) total score, nausea and fullness subscales, upper abdominal pain score, gastroesophageal reflux disease score, and the patient assessment of upper GI disorders—quality-of-life score.
In a systematic review (113) of 14 studies that evaluated GE and upper GI symptoms, including IG or DG, and including only studies with optimal GE test methods being evaluated, there was a significant positive association between improvements in GE and upper GI symptoms in response to prokinetic agents.
Immunological therapies
There is insufficient evidence to support routine clinical use of autoimmune therapies in management of GP. A retrospective analysis of 11 female patients (114) with drug- and device-resistant GP with coexisting positive autoimmune profiles who were treated for 8–12 weeks with diverse immunomodulatory treatment showed that total symptom score improved in 6 of 11 patients, with maximum GI symptom improvement with intravenous immunoglobulin (IVIg) (2 of the 3 patients treated). In a subsequent open-label study, 14 patients (3 DG, 1 PSG, and 10 IG) with serological and/or tissue evidence of immunological abnormality, IVIg therapy (400 mg/kg infusion weekly for 12 weeks) was associated with significant improvement in symptoms scores for nausea, vomiting, early satiety, and abdominal pain, and 9/14 patients were responders to this open-label treatment (115). This study built on the retrospective medical record review, suggesting a positive experience among 11 patients treated with IVIg or combined mycophenolate mofetil with methylprednisolone or only mycophenolate mofetil therapy (114).
Nonpharmacological therapy for GP: GES, acupuncture, and herbal medicines
Recommendation
- 15. Gastric electric stimulation (GES) may be considered for control of GP symptoms as a humanitarian use device (HUD) (conditional recommendation, low quality of evidence).
GES is approved as an HUD, as defined by the FDA for medically refractory DG or IG. The recommendation includes the use of GES in humanitarian use.
Table 7 shows efficacy of several bioelectric treatments including vagal nerve stimulation, spinal cord stimulation, and GES (116–141). A recent randomized, crossover trial of ON vs OFF GES in patients with medically refractory vomiting with or without delayed GE, GES decreased the vomiting frequency. Severity of nausea and appetite improved while ON compared with OFF. However, there were no differences in GI quality of life, nutritional parameters, or GE (120). Randomized, crossover trials of GES for medically refractory DG or IG have shown mixed results, which may reflect the variation in trial designs with differing timing of the ON vs OFF randomization and crossover (119–123). Other modalities of electrostimulation (vagal and spinal cord) seem promising; however, larger randomized, sham-controlled trials are needed to determine the efficacy. However, documented clinical usefulness in both IG and DG (documented in Table 7) suggests there is a role for GES in accordance with its HUD approval.

Efficacy of several bioelectric therapies in GP
Recommendations
- 16. Acupuncture alone or acupuncture combined with prokinetic drugs may be beneficial for symptom control in patients with DG. Acupuncture cannot be recommended as beneficial for other etiologies of GP (conditional recommendation, very low quality of evidence).
- 17. Herbal therapies such as Rikkunshito or STW5 (Iberogast) should NOT be recommended for treatment of GP (conditional recommendation, low quality of evidence).
Table 8 summarizes information on effects of electroacupuncture, acupuncture, and herbal medicines in GP (142–153). The evidence available does not support their use in clinical practice.

Effect of electroacupuncture, acupuncture, and herbal medicines in GP
Pyloric interventions: diagnostic and therapeutic
Recommendations
- 18. In patients with GP, EndoFLIP evaluation may have a role in characterizing pyloric function and predicting treatment outcomes after peroral pyloromyotomy (conditional recommendation, very low quality of evidence).
- 19. Intrapyloric injection of botulinum toxin is not recommended for patients with GP based on randomized, controlled trials (strong recommendation, moderate quality of evidence).
- 20. In patients with GP with symptoms refractory to medical therapy, we suggest pyloromyotomy over no treatment for symptom control (conditional recommendation, low quality of evidence).
Table 9 shows results of EndoFLIP for selection of patients for pyloromyotomy or pyloric botulinum toxin injection (154–160). Current evidence suggests that such measurements of pyloric diameter and distensibility index or compliance are associated with greater gastric retention, and that the measurements may predict response to therapy, particularly, significant enlargement of the post–G-POEM pyloric diameter (158). It is reasonable to consider such pyloric interventions in a clinical trial and to include assessments of pyloric physiology to appraise the impact of pyloric dysfunctions on outcomes. Thus, although intrapyloric injection of botulinum toxin is not recommended for patients with GP based on randomized, controlled trials (161), a recent large multicenter study from France documents the efficacy of botulinum toxin injection, particularly for the relief of vomiting, when patients are selected based on measurements of pyloric distensibility (160).

EndoFLIP for selection of patients for pyloromyotomy or pyloric botulinum toxin injection
Efficacy of G-POEM for GP based on open-label studies
Table 10 shows efficacy of G-POEM for GP based on open-label studies (162–180). Overall, these open-label studies suggest there is benefit in terms of symptom improvement and improved GE, although most studies were of only 3–6 months’ duration. A 12-month study showed 56% patients improved at 1 year (172). Symptom control after endoscopic pyloromyotomy is comparable with surgical myotomy; however, endoscopic myotomy has been associated with fewer postprocedural complications and shorter length of hospital stay. A recent study has identified benefit in relief of symptoms as well as improved GE with G-POEM procedure followed for 6 months in a sham-controlled study (173). Other pylorus-directed procedures are also available such as surgical pyloroplasty, although there is more evidence on G-POEM. Heineke-Mikulicz pyloroplasty involves longitudinal incision across the pylorus, which is then closed transversely, and this results in division of both longitudinal and circular muscle layers. In 177 patients with GP, laparoscopic pyloroplasty achieved improved GE in 90% of patients and induced short-term improvement of nausea, vomiting, bloating, and abdominal pain. However, morbidity rate was 6.8%, with problems such as confirmed leaks or further surgical interventions including jejunostomy and subtotal gastrectomy (181).

Efficacy of G-POEM for gastroparesis based on open-label studies
CONCLUSION AND A LOOK TO THE FUTURE
This guideline has focused on the diagnosis and treatment of GP in adults (including dietary, pharmacological, device, and interventions directed at the pylorus). The recommendations made are guided by assessment using GRADE methodology. Nevertheless, this is an area with considerable ongoing innovation, validation, and research that is likely to impact future iterations of these guidelines. In particular, the following have potential future impact on the management of GP: The diagnostic value of WMC for GP and for measurements of pan-GI transit and pressure profiles and autonomic nervous system dysfunction are under investigation. Similarly, studies are exploring the optimal approaches to select and individualize patients for treatments including documentation of circulating antibodies, measurements of the pylorus and high-resolution antropyloroduodenal manometry, extensive surface EGG (high-resolution electrical mapping), and full-thickness antral and pyloric biopsies. Such advances should clarify the role of immunotherapies, novel pharmacological agents, pyloric interventions, bioelectric therapy, and surgical approaches for GP.
CONFLICTS OF INTEREST
Guarantor of the article: Michael Camilleri, MD, DSc, MACG.
Specific author contributions: All authors contributed to researching, writing, and editing this manuscript. Drs. Abell and Camilleri serve as senior authors of the manuscript.
Financial support: MC receives NIH funding for studies on gastroparesis (R01-DK122280 and R01-DK125680). TA receives NIH funding for gastroparesis (7U01-DK074007–07 and R56DK126935). BK receives NIH funding for gastroparesis (R21-DK116029 and U01-DK112193); NIDDK Diabetic Complications Consortium (DK076169, DK115255). LN receives support for research by a philanthropic gift from Colleen and Robert D. Hass.
Potential competing interest: MC: single-center research studies: Allergan, Takeda, and Vanda; consulting with compensation to his employer: Takeda and Alpha Sigma Wasserman. TA: investigator: Censa, Cindome, Vanda, Allergan, and Neurogastrix; consultant: Censa, Nuvaira, Takeda, and Medtronic; speaker: Takeda and Medtronic; reviewer: UpToDate; writer: Med Study; editorial: Neuromodulation, Wikistim; ADEPT-GI: IP for autonomic/enteric diagnosis and therapies. BK: clinical trials with Takeda, Vanda, and Alpha Sigma Wasserman, GSK; consulting with Takeda, Cindome, and Neurogastrix; speaking for Medtronic. LN: investigator: Allergan and Vanda; consultant: AbbVie, Ironwood, Alnylam, Eli Lilly, Evoke, Gemelli, Neurogastrx, Pendulum, Phathom, RosVivo, Salix, and Takeda. Scientific advisory board: Gemelli and RosVivo. VMV: nothing to disclose. JP: nothing to disclose. KG: nothing to disclose. RY: consultant through institutional agreement: Medtronic, Ironwood Pharmaceuticals, Diversatek, and StatLinkMD; research support: Ironwood Pharmaceuticals; advisory board: Phathom Pharmaceuticals; RJS Mediagnostix.
Acknowledgements
The authors thank Dr. David Armstrong (McMaster University, Hamilton, Ontario, Canada) for participation in the initial literature reviews, Dr. Prateek Mathur (University of Louisville, Kentucky) for assistance with some of the tables in the article, and Mrs. Cindy Stanislav for excellent secretarial assistance.
REFERENCES





