Antibiotics With or Without Rifaximin for Acute Hepatic Ence… : Official journal of the American College of Gastroenterology
INTRODUCTION
Hepatic encephalopathy (HE) is a potentially reversible complication of liver failure that is characteristically associated with varying degrees of cognitive decline, ranging from minor attention deficits to gross disorientation and coma (1). HE is a common reason for hospitalization, and patients with overt HE usually require intensive care unit (ICU) admission for appropriate management (2,3). Management of acute HE is focused on identifying and addressing the precipitating event while concomitantly reducing the levels of ammonia and endotoxins using various measures (4). There are several pharmacologic strategies used for the treatment of acute HE, which includes disaccharidases (lactulose), polyethylene glycol, nonabsorbable antibiotics (ab), zinc, L-ornithine L-aspartate (LOLA) infusion, and ornithine phenylacetate (5–7). However, lactulose is currently the only recommended drug of choice for the treatment of acute HE (8–10). LOLA infusions and polyethylene glycol are suggested for patients who are nonresponsive or intolerant to lactulose (9).
Rifaximin is an excellent antibiotic with coverage against Gram-positive and -negative bacteria (11). It reduces the load of gut-derived toxins, in addition to reducing proinflammatory cytokine levels. In addition, although rifaximin does not seem to change the overall bacterial composition of the gut microbiota, it seems to modulate the function of the gut microbiota (12,13). Rifaximin is approved for the treatment of travelers’ diarrhea caused by noninvasive strains of Escherichia coli, small intestinal bacterial overgrowth, treatment of irritable bowel syndrome with diarrhea, and last, for recurrent overt HE (8,14–16). Previous studies reported significantly lower mortality and shorter hospitalization in patients with HE because of lesser incidence of sepsis in patients treated with a combination of rifaximin, lactulose, and LOLA (17,18). However, rifaximin has not yet been approved by the US Food and Drug Administration for the treatment of acute overt HE owing to the limited number of studies that provided evidence of its efficacy for acute HE. Despite not being endorsed by current practice guidelines, rifaximin is widely used in ICU settings to treat overt HE. It is pertinent to note that patients with overt HE admitted to the ICU often receive broad-spectrum ab superior to rifaximin. A combination of intravenous ceftriaxone, LOLA, and lactulose leads to an ill-sustained improvement in the grade of HE (19). However, the potential synergistic effect of rifaximin in patients receiving systemic ab and its role in preventing endotoxin rise acting locally in the gut remains unclear. Furthermore, no existing studies have compared the efficacy of broad-spectrum ab with or without rifaximin in treating overt HE in critically ill patients with cirrhosis, which we aimed to assess in this randomized controlled trial.
METHODS
Study design
This prospective, single-center, double-blind randomized controlled trial aimed to evaluate the efficacy of broad-spectrum ab with or without rifaximin in treating patients with cirrhosis with overt HE in the ICU. Patients were enrolled at the Asian Institute of Gastroenterology Hospital, Gachibowli, Hyderabad, India, from February 28, 2022, to April 3, 2023. The primary objective was to compare the proportion of patients achieving 2-grade reduction and/or complete resolution of HE between patients who received ab alone and those who received antibiotics + rifaximin. Key secondary objectives was to compare the time taken to achieve 2-grade HE reduction or resolution, in-hospital mortality, duration of hospital stay, incidence of nosocomial infections, and endotoxin levels at baseline and after achieving the primary objective between the 2 groups. We also analyzed the predictors of HE resolution and assessed the effects of rifaximin in patients with decompensated cirrhosis (DC) and acute-on-chronic liver failure (ACLF). The study protocol was approved by the institutional ethics committee (AIG/IEC- BH&R 24/02.2022–01) and was conducted in accordance with the modified Declaration of Helsinki. Informed consent was obtained from the patient’s responsible representative. The study was registered with the Clinical Trials Registry–India (CTRI/2022/03/041210).
Patients
Consecutive adult patients aged 18–75 years with overt HE (≥grade 2) with a background of liver cirrhosis admitted to the ICU were screened for recruitment within 24 hours of admission. Patients with acute liver failure; patients with blood urea level> 150 mg/dL (normal range: 17–43 mg/dL); West-Haven grade 1 HE; underlying chronic kidney disease (CKD); hepatocellular carcinoma; patients with an underlying neuropsychiatric disease or those receiving antidepressants or antipsychotics medications; patients with acute cerebrovascular events including intracranial hemorrhage, thrombosis or space-occupying lesions; patients with a (<1 week) history of alcohol consumption; and those who died within 24 hours of ICU admission (before randomization) were excluded.
Intervention, management, and follow-up
Patients in group I received only ab, and patients in group II received rifaximin in addition to ab. The use of cephalosporins, penicillin with beta-lactamase inhibitors, carbapenems, fluoroquinolones, macrolides, and glycopeptides were considered as broad-spectrum ab. Rifaximin (550 mg) was administered orally or through a nasogastric tube twice daily for 14 days or until death or discharge, whichever occurred first. All patients received standard medical therapy, which included lactulose solution or enema to ensure 2–3 soft stools/d (8–10). Underlying precipitants, such as dyselectrolytemia, infection, and variceal bleeding, were treated according to the hospital protocol. Diuretics were withheld. Patients with acute kidney injury (AKI) received terlipressin therapy (unless contraindicated) in addition to volume expansion through albumin infusions; these patients did not receive LOLA infusions owing to a lack of safety data. All patients with grade 4 HE underwent a noncontrast computed tomography scan of the brain to rule out intracranial pathology as per hospital policy. West-Haven criteria were used for grading HE (8). The assessment of HE in our study adhered to a rigorous and standardized protocol, which aligns with the routine clinical practice in our ICU. HE was assessed once daily between 9 and 10 am consistently throughout the entire study period. To ensure the reliability and validity of our HE assessments, we set up a team of 2 medical professionals (M.A. and P.K.) responsible for conducting the initial assessments. In cases where a consensus on the HE grade was not reached between the 2 assessors, a third expert (A.V.K.) was consulted to adjudicate and establish a definitive HE grade. For patients on mechanical ventilation (intubated), HE assessments were performed daily following the withdrawal of sedative drugs in the morning. Patients underwent complete clinical examination, chest radiography, ascitic fluid analysis, and blood and urine culture examinations at baseline to identify infection. These tests were repeated whenever a patient exhibited signs and symptoms suggestive of infection. Endotoxin levels were assessed on day 1 of inclusion and at the time of resolution of HE using a Pierce Chromogenic Quant kit (Thermo Fisher Scientific), and the values were expressed as EU/mL (Detailed methodology in Supplementary Digital Content 1, https://links.lww.com/AJG/D109). These endotoxin levels were assessed by V.S. and D.G., who were blinded to the treatment groups. Patients were followed up by 2 investigators (P.K. and K.R.) until discharge.
Definitions
Liver cirrhosis was based on a history of decompensations (ascites, HE, or variceal bleeding) with imaging (altered echotexture, dilated portal vein, or splenomegaly) or biopsy evidence of cirrhosis. ACLF was defined according to the Asian Pacific Association for the Study of the Liver (APASL) criteria. Patients with a history of DC and/or those who did not meet the criteria of APASL ACLF were labelled as DC (20). Development of HE within 4 weeks of onset of jaundice in the absence of prior underlying liver disease was labelled as acute liver failure (21). Patients with a glomerular filtration rate of less than 60 mL/min per 1.73 m2—or markers of kidney damage, or both—for at least 3 months duration or those with known CKD regardless of the underlying cause were labelled as CKD (22). Infections were defined according to standard definitions (23,24). AKI was defined as an increase in serum creatinine by 0.3 mg/dL within 48 hours or a 50% increase from baseline, which is presumed or known to have occurred within 7 days earlier (25).
Sample size
Previous reports have demonstrated that resolution of HE occurs in up to 92.5% of patients receiving rifaximin, LOLA, and lactulose (18). Considering that this combination, in addition to broad-spectrum ab, will be as effective as broad-spectrum ab alone (or at least noninferior) with a power of 90% and an alpha error of 5% and with a margin of 15% in HE resolution, we needed to enroll 88 patients in each arm. Furthermore, considering a 5% attrition rate, we needed 92 patients in each arm. Thus, we planned to include 184 patients with acute HE in this study. Computer-generated randomization charts were used to randomize patients into 2 arms of the study in a 1:1 ratio to receive broad-spectrum ab alone or broad-spectrum ab and rifaximin. Patients were enrolled and assigned to each arm as per the generated randomization sequence by the clinical trial coordinators (R.N. and S.S.) using the sequentially numbered opaque sealed envelope method. The trial investigators (A.V.K. and A.G.) and patients were blinded to the randomization.
Statistical analysis
All patients who were randomized and received a single dose of ab with or without rifaximin were included in the analysis and analyzed per the intention-to-treat principle. A per-protocol analysis was also performed for major outcomes. Descriptive statistics are presented as mean (SD) and median (interquartile range) for parametric and nonparametric continuous data, respectively, and as proportion (n, %) for categorical data. The Student t test was used for comparisons between continuous data, whereas the χ2 test or Fisher exact test (if any of the values in the 2 × 2 table was less than 5) was used for categorical data to compare the proportions. A Kaplan-Meier survival analysis was used to assess the resolution of HE and in-hospital mortality. A stepwise univariate and multivariate Cox regression analysis was performed to determine the predictors of HE resolution and reported as hazard ratio (HR) with a 95% confidence interval (CI). A receiver operative characteristic curve analysis was performed to identify the ideal cut-off for predictors that were significant in a multivariate analysis. Statistical significance was defined as P < 0.05 for all tests. SPSS version 29.0 (IBM, Armonk, NY) was used for all statistical analyses.
RESULTS
Patient characteristics
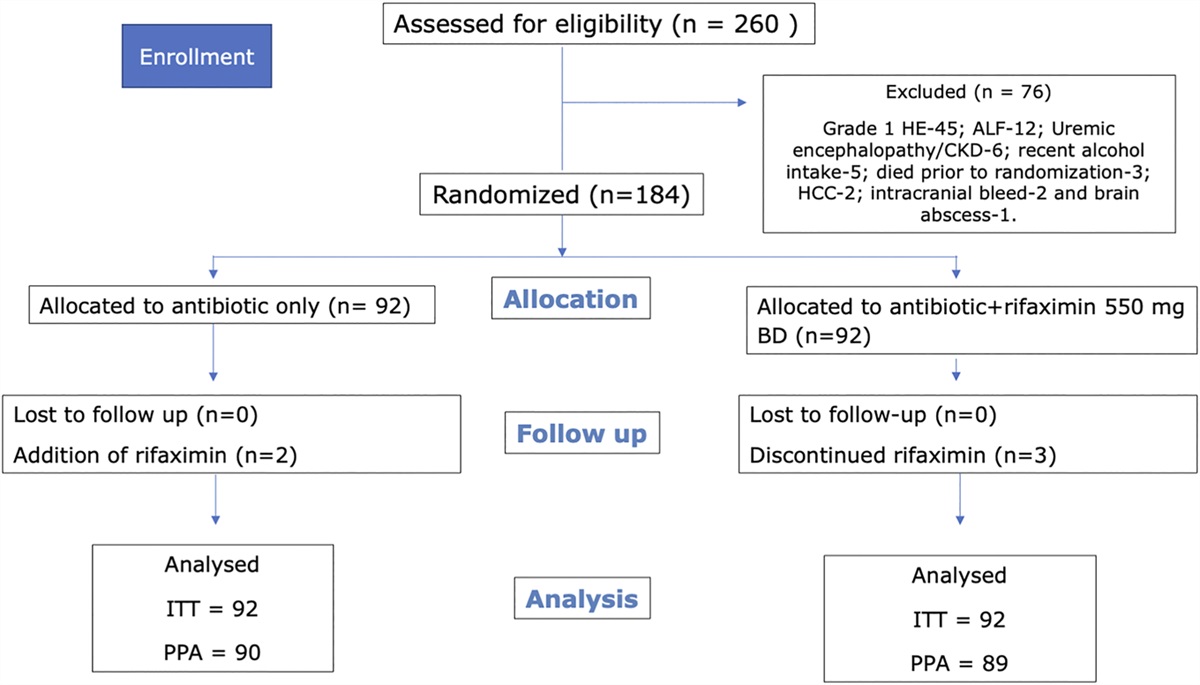
A total of 260 patients were screened for inclusion in the study. Seventy-six patients were excluded because of various reasons (Figure 1). Two patients in the antibiotic-only group received rifaximin after enrolment because of nonresponse after 4 days; however, these patients were included in the antibiotic-only group on intention-to-treat analysis. Thus, 184 patients, 92 in each group, were included in the analysis. The mean age, sex distribution, grades of HE, and severity scores were similar among both groups (Table 1). Most of the patients were men (approximately 90%), and alcohol was the most common etiology of liver disease. The most common precipitant of HE was constipation with dyselectrolytemia in both groups (41%). Sixty-one percent in the antibiotic-only group and 50% in the ab + r group had AKI at baseline (P = 0.18). Forty-six percent in the antibiotic-only group and 40.2% in the ab + r group had an infection at baseline (see Table, Supplementary Digital Content 2, https://links.lww.com/AJG/D110). Fifty-two percent of patients (96/184) were identified as ACLF as per the APASL criteria. The proportions of patients with ACLF in both groups was similar (50% vs 54.3%; P = 0.55).

Consort chart. ACLF, acute-on-chronic liver failure; BD, twice a day; CI, confidence interval; CKD, chronic kidney disease; DC, decompensated cirrhosis; HCC, hepatocellular carcinoma; HE, hepatic encephalopathy; HR, hazard ratio; ITT, intention to treat; PPA, per protocol analysis.

Baseline characteristics of patients included in the study
Two-grade reduction (improvement) in HE and/or complete resolution of HE.
The median number of stools passed per day in both groups was similar (4 [0–6] in ab arm vs 4 [2–6] in ab + r group; P = 0.86). On Kaplan-Meier analysis, 44.6% (41/92; 95% CI, 32–70.5) in ab-only arm and 46.7% (43/92; 95% CI, 33.8–63) in ab + r arm achieved the primary objective (P = 0.84) (see Figure a, Supplementary Digital Content 3, https://links.lww.com/AJG/D111). Time to achieve the primary objective was 3.65 ± 1.82 days in the ab-only arm and 4.11 ± 2.01 days in the ab + r arm (P = 0.27). The resolution of HE in patients with infection (31% [13/42] vs 35.1% [13/37]; P = 0.7) and without infection (56% [28/50] vs 54.5% [30.55]; P = 0.88) was similar in both groups.
In-hospital mortality.
On Kaplan-Meier analysis, the in-hospital mortality was 62% (57/92; 95% CI, 47–80) in ab-only arm and 50% (46/92; 95% CI, 36.6–66.7) in ab + r arm (P = 0.06) (Figure 2). The most common cause of mortality was sepsis with multiorgan dysfunction, followed by progressive liver failure in both groups (see Table, Supplementary Digital Content 4, https://links.lww.com/AJG/D112). In-hospital mortality rate was comparable among those with (73.8% [31/42] vs 59.5% [22/37]; P = 0.17) and without infection among both groups (52% [26/50] vs 43.6% [24/55]; P = 0.39).

Kaplan-Meier survival analysis among antibiotic alone and antibiotics + rifaximin arm. CI, confidence interval; HR, hazard ratio.
Duration of hospital stay.
The mean duration of hospital stay was comparable between the 2 groups (8.9 ± 6.38 days in the ab-only group vs 10.15 ± 6.52 days in the ab + r group; P = 0.18).
Incidence of nosocomial (new-onset in-hospital) infection.
Six (6.5%) and 12 patients (13%) in antibiotic-only arm and ab + r arm, respectively, developed nosocomial infections (P = 0.21). The most common site of infection in both groups was the lungs, and Klebsiella was the most commonly isolated organism. Twelve percent (11/92) in the ab-only group and 14.1% (13/92) in the antibiotics-rifaximin group (P = 0.82) needed the addition of another systemic antibiotic or an upgrade to carbapenems. Table 2 highlights the sites of nosocomial infections and isolated organisms. Among the patients who already had an infection at baseline, the resolution of infection was achieved in a similar proportion of patients in the ab (40.5%; 17/42) arm and ab + r arm (43.2%; 16/37; P = 0.49).

Site of nosocomial infection and organisms isolated
Change in endotoxin levels.
At baseline, the endotoxin levels were similar in both groups (1.22 ± 0.72 EU/mL vs 1.3 ± 0.86 EU/mL; P = 0.8). Furthermore, at the time of achieving the primary objective, the endotoxin levels were comparable among both groups (1.3 ± 1.2 EU/mL vs 1.2 ± 0.82 EU/mL; P = 0.93). The endotoxin levels in the ab arm remained the same/increased, whereas the endotoxin levels in ab + r group declined, although the difference was not statistically significant (0.08 ± 0.76 EU in the ab arm vs −0.01 ± 0.43 EU/mL in ab + r group; P = 0.64) (Figure 3).

Change in endotoxin levels in each group at hepatic encephalopathy resolution.
Predictors of 2-grade reduction in HE/resolution of HE.
There were several variables, including age, use of LOLA, infection at baseline, DC vs ACLF, total leukocyte counts, bilirubin, albumin, INR, blood urea levels, and severity scores (Model for End-stage Liver Disease [MELD], MELD-Na, and Sequential Organ Failure Assessment [SOFA] score) which predicted 2-grade reduction/complete resolution of HE. However, on a multivariate Cox regression analysis, only serum bilirubin levels (HR, 0.96 [0.94–0.99]; P = 0.005), serum albumin levels (HR, 1.68 [1.12–2.5]; P = 0.01), and SOFA score (HR, 0.88 [0.82–0.95]; P = 0.002) at admission predicted 2-grade reduction/resolution of HE (Table 3). On the receiver operative characteristic analysis, SOFA score ≤9.5 and serum bilirubin ≤15.45 mg/dL predicted HE reduction/resolution with an area under the curve of 0.71 (95% CI, 0.64–0.78; P < 0.001) and 0.64 (0.56–0.72; P < 0.001), respectively. However, a serum albumin level ≥2.5 g/dL could predict HE reduction/resolution with an area under the curve of 0.64 (95% CI, 0.55–0.72; P = 0.001) (see Figure, Supplementary Digital Content 5, https://links.lww.com/AJG/D113).

Predictors of 2 grade reduction/resolution of HE on stepwise univariate and multivariate Cox regression analysis
Adverse events.
Two patients complained of itching and 1 of bloating and loose stools in the rifaximin arm and were discontinued after 7 days of therapy. There were no other significant severe drug-related adverse events.
Subgroup analysis of DC and ACLF
DC.
Of the 88 patients with DC, 46 received ab alone and 42 received ab and rifaximin. Baseline variables, including demographics, biochemical variables, grade of HE, and severity scores, were comparable between patients with DC receiving ab and ab + r (see Table, Supplementary Digital Content 6, https://links.lww.com/AJG/D114). On Kaplan-Meier analysis, 47.8% [22/46] in the ab-only arm compared with 64.3% [27/42] in the ab + r arm achieved the primary objective (P = 0.16) (see Figure b, Supplementary Digital Content 3, https://links.lww.com/AJG/D111). The time to achieve the primary objective was similar among both groups (2.95 ± 1.13 days vs 3.7 ± 2.14; P = 0.14). The median number of stools passed per day was also similar (4 [2–5] vs 4 [2–5]; P = 0.96). On Kaplan-Meier analysis, in-hospital mortality was 56.5% (26/46; [95% CI, 37–82.8]) in patients with DC receiving only ab compared with 33.3% (14/42; [95% CI, 18.2–56]; P = 0.003) in those receiving additional rifaximin (Figure 4a). The proportion of patients achieving the resolution of infection was similar (56.3% vs 43.8%; P = 0.48). However, the development of nosocomial infections was higher in ab-alone group (10.86% [5/46]) compared with ab + r group (0%; P = 0.02), and 60% (3/5) of those with nosocomial infection died in-hospital. The sites of infection were the lungs (n = 2), urinary tract, bacteremia, and skin and soft tissue (n = 1 each). Both groups had a comparable decline in the endotoxin levels (−0.2 ± 0.41 in ab vs −0.13 ± 0.33 EU/mL in ab + r group; P = 0.66). The proportion of patients achieving HE resolution (31.3% [5/16] vs 50% [8/16]) and mortality (75% [12/16] vs 50% [8/16]; P = 0.14) was similar with rifaximin in patients with infection at baseline. Although in patients without infection at baseline, the resolution of HE was comparable (56.7% [17/30] vs 73.1% [19/26]; P = 0.2) but mortality was lower (46.7% [14/30] vs 23.1% [6/26]; P = 0.06) with rifaximin use.

Kaplan-Meier in-hospital survival among patients with (a) decompensated cirrhosis and (b) acute-on-chronic liver failure (ACLF). CI, confidence interval; HR, hazard ratio.
ACLF.
Of the 96 patients with ACLF, 46 received ab alone and 50 received ab + r. Baseline variables, including demographics, biochemical variables, grade of HE, and severity scores among patients with ACLF receiving ab and ab + r, were comparable among the 2 groups (see Table, Supplementary Digital Content 6, https://links.lww.com/AJG/D114). On Kaplan-Meier analysis, 41.3% (19/46) in the ab arm compared with 32% (16/50) in the ab + r arm achieved the primary objective (P = 0.34), and the time taken was also comparable (4.47 ± 2.14 vs 4.81 ± 1.6; P = 0.6) (see Figure c, Supplementary Digital Content 3, https://links.lww.com/AJG/D111). The median number of stools passed per day was similar (4 [0–6] vs 4 [2–6]; P = 0.84). On Kaplan-Meier analysis, in-hospital mortality was 67.4% (31/46; [95% CI, 45.8–95.6]) in the control arm compared with 64% (32/50 [95% CI, 43.8–90.3]; P = 0.98) in patients with ACLF receiving rifaximin (Figure 4b). The proportion of patients achieving infection resolution was also comparable (61.5% [16/26] vs 66.7% [14/21]; P = 0.71). Nine percent (4/46) in the ab-alone group and 18% (9/50) in ab + r group developed nosocomial infections (P = 0.23). All the patients with nosocomial infection died in-hospital. The resolution of HE, infections, and in-hospital mortality was similar, irrespective of the grade of ACLF and the presence or absence of infection at baseline. There was a comparable increase in the endotoxin levels in both groups (0.8 ± 1 in ab-only group vs 0.21 ± 0.56 EU/mL in ab + r group; P = 0.3).
Per protocol analysis
There were 5 patients (2 in the ab arm and 3 in the ab + r arm) who had protocol deviations. All these patients had ACLF. There was no impact on resolution of HE or in-hospital mortality even on per protocol analysis (see Figure, Supplementary Digital Content 7, https://links.lww.com/AJG/D115).
DISCUSSION
The key results of this study indicate that the addition of rifaximin to broad-spectrum antibiotic therapies does not result in early HE resolution and does not reduce the incidence of infections or endotoxin levels. The study highlights that serum albumin and SOFA score are important predictors of HE resolution in critically ill patients with cirrhosis admitted to ICU. These results prompt a critical re-evaluation of rifaximin’s clinical benefits in ICU settings, urging further exploration of alternative approaches to advance the management of overt HE in critically ill patients.
Rifaximin has limited systemic absorption and is excreted unchanged in stools and is characteristically known to have fewer adverse effects with good tolerability and minimal drug interactions (26). Rifaximin enhances the intestinal epithelial layer homeostasis, favorably alters the gut microbiota, reducing the ammonia-producing colonic bacteria, and leading to a reduction in ammonia levels (26,27). A previous study reported a reduction in the incidence of sepsis in patients with HE and led to early recovery and reduced mortality rates (17). However, high-quality evidence that supports the use of rifaximin for the prevention of bacterial infections, including spontaneous bacterial peritonitis, is lacking (28,29).
Infection is a common reason for ICU admission, and infection caused by multidrug-resistant organisms is a unique challenge in these patients (30). In this study, 40% of the patients had an infection at baseline and were on systemic ab. Furthermore, these patients were quite ill and had high MELD and SOFA scores; therefore, <50% could achieve HE resolution. Therefore, rifaximin may not have been effective in reducing the occurrence of infection or controlling sepsis. Although we noted a decrease in the incidence of nosocomial infections and improved survival in patients with DC, there was no significant impact on the resolution of HE with rifaximin. Rifaximin is also known to have minimal effects on bacterial translocation and inflammatory markers, which was also observed in this study upon assessment of endotoxin levels (31). Furthermore, it is well known that HE in patients with ACLF is more related to cytokine storm, inflammation, and endotoxemia, which rifaximin cannot alter (32).
We noted that serum albumin levels, bilirubin levels, and SOFA score played a crucial role in predicting the improvement/resolution of HE. Lower serum albumin levels predict poorer cognitive function because of endothelial dysfunction and increased oxidative stress (30,33). Prophylactic albumin infusions have been reported to improve cognitive function and psychosocial quality of life in patients with a history of HE or minimal HE (33). Furthermore, albumin infusions, in addition to lactulose, is more effective in reversing overt HE over lactulose alone (34). High serum bilirubin level suggests advanced liver disease and is a marker of short-term mortality in hospitalized patients (35,36). SOFA score has been validated to predict poor prognosis in patients admitted to ICU and is a component of ACLF scoring systems (30,37,38). Given that we included ICU patients in this study, the results confirm that SOFA score is strongly associated with the prediction of HE resolution (39).
The population of this study included mostly men and those with alcohol-related cirrhosis. Long-term rifaximin administration suppresses inflammation and prevents the progression of fibrosis in patients with alcohol-related liver diseases (26,40,41). However, short-term rifaximin administration has minimal effects, even in patients with alcohol-related liver cirrhosis (31,42). Sex-based differences in gut microbiota composition in patients with HE are well known (43). Although gender-based difference in outcomes has not been reported with rifaximin, it may be worthwhile to test rifaximin in women with different etiology of liver cirrhosis. Last, patients with alcohol-related liver diseases are prone to fungal infections and infections caused by multidrug-resistant organisms, which may partially explain the ineffectiveness of rifaximin (23,44).
In this study, ab were administered in accordance with the hospital protocol for clinically suspected sepsis. The alarming increase in cases of infections caused by multidrug-resistant organisms significantly affects our decision-making regarding antibiotic selection (45). In particular, it necessitates the use of potent ab in an attempt to combat these increasingly resistant pathogens. It may be argued that the cost of systemic ab is higher than rifaximin; however, rifaximin is not inexpensive. Accordingly, its inclusion is unwarranted and impractical if evidence supporting its substantial clinical benefits are lacking. Considering that even a modestly priced drug (such as rifaximin) holds significance for patients with budget constraints, prioritizing resources for medications with proven efficacy and greater impact on patient outcomes reflects clinical prudence and responsible financial management.
This study has a few limitations. First, LOLA, which is reported to be effective in reversing HE, was not administered to all the patients. The limited use of LOLA was because of the lack of strong recommendations for its use; however, it was selectively administered to <50% of the patients without kidney injury. Second, HE was assessed at fixed hours in the morning. This may have led to an underestimation of the exact time to HE resolution. Third, the lack of a placebo group may have affected the conclusions of this study. However, we considered a noninferiority trial with a decent sample size because rifaximin is easy and safe to administer in critically ill patients in ICU, and the results would not have differed from those of a study with a placebo group. Finally, the study cohort included sick patients with high severity scores, and the benefit of rifaximin in less sick patients admitted to a non-ICU setting may differ.
In conclusion, this study demonstrated that rifaximin does not significantly contribute to the resolution of HE in critically ill patients with cirrhosis who are admitted to the ICU and are already receiving lactulose and other ab, which often offer a comparable or superior spectrum of action.
CONFLICTS OF INTEREST
Guarantors of the article: Anand V. Kulkarni, MD, DM, and Padaki Nagaraja Rao, MD, DM.
Specific author contributions: A.V.K., A.G., D.N.R., and P.N.R.: conceptualization. A.V.K. and M.S.: methodology. D.N.R. and P.N.R.: software. A.V.K., S.V., and M.A.: formal analysis. M.A., P.K., R.N., S.S., and A.A.Z.: investigation and data curation. D.N.R.: resources. V.S. and D.G.: Biochemical tests. M.A. and A.V.K.: writing original draft. A.V.K., A.G., S.I., M.P.K. and K.R.R.: writing, reviewing, and editing. D.N.R. and P.N.R.: supervision. A.V.K. and A.G.: project administration.
Financial support: None to report.
Potential competing interests: None to report.
Data availability: Data will be provided on a reasonable request to the corresponding author with scientific rationale.
Ethics (IRB) approval: Obtained.
Study Highlights
WHAT IS KNOWN
- ✓ Hepatic encephalopathy (HE) is a common indication for intensive care unit admission.
- ✓ Critically ill patients with cirrhosis in the intensive care unit usually receive broad-spectrum antibiotics.
- ✓ Rifaximin prevents the recurrence of HE.
WHAT IS NEW HERE
- ✓ Rifaximin does not lead to early resolution of HE in critically ill patients with cirrhosis.
- ✓ Rifaximin does not reduce the rate of nosocomial infections.
- ✓ Rifaximin may reduce rates of nosocomial infections and in-hospital mortality in patients with decompensated cirrhosis.
- ✓ Rifaximin has no effect in patients with acute-on-chronic liver failure.
ACKNOWLEDGEMENTS
We thank Prof. K. Rajender Reddy for meticulously assessing the manuscript.
REFERENCES
Discover more from reviewer4you.com
Subscribe to get the latest posts to your email.





